
Page 50 - Summer 2017 Journal
P. 50
DIFFERENT PARADIGMS
Let’s start by looking at the conventional explanation of a heart attack.
I learned in medical school that there are four major coronary arteries leading to different areas of the heart. Interestingly, Wikipedia says that there are only three, and some cardiology books say there are just two. You would think that we would know for certain how many coronary arteries there are. (Actually, nobody disputes the anatomy—two main coronary arteries that branch—but there is a somewhat semantic debate about whether also to count the ones that branch as main arteries.)
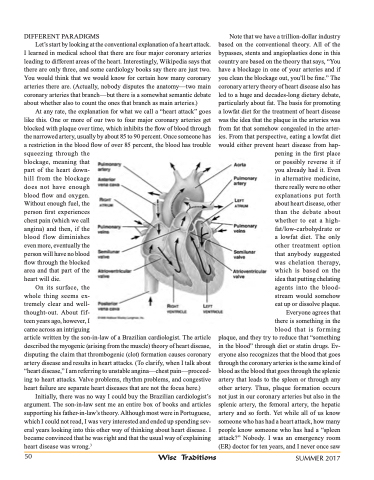
At any rate, the explanation for what we call a “heart attack” goes like this. One or more of our two to four major coronary arteries get blocked with plaque over time, which inhibits the flow of blood through the narrowed artery, usually by about 85 to 90 percent. Once someone has a restriction in the blood flow of over 85 percent, the blood has trouble squeezing through the
blockage, meaning that
part of the heart down-
hill from the blockage
does not have enough
blood flow and oxygen.
Without enough fuel, the
person first experiences
chest pain (which we call
angina) and then, if the
blood f low diminishes
even more, eventually the
person will have no blood
flow through the blocked
area and that part of the
heart will die.
On its surface, the
whole thing seems ex-
tremely clear and well-
thought-out. About fif-
teen years ago, however, I
came across an intriguing
article written by the son-in-law of a Brazilian cardiologist. The article described the myogenic (arising from the muscle) theory of heart disease, disputing the claim that thrombogenic (clot) formation causes coronary artery disease and results in heart attacks. (To clarify, when I talk about “heart disease,” I am referring to unstable angina—chest pain—proceed- ing to heart attacks. Valve problems, rhythm problems, and congestive heart failure are separate heart diseases that are not the focus here.)
Initially, there was no way I could buy the Brazilian cardiologist’s argument. The son-in-law sent me an entire box of books and articles supporting his father-in-law’s theory. Although most were in Portuguese, which I could not read, I was very interested and ended up spending sev- eral years looking into this other way of thinking about heart disease. I became convinced that he was right and that the usual way of explaining heart disease was wrong.3
50
Note that we have a trillion-dollar industry based on the conventional theory. All of the bypasses, stents and angioplasties done in this country are based on the theory that says, “You have a blockage in one of your arteries and if you clean the blockage out, you’ll be fine.” The coronary artery theory of heart disease also has led to a huge and decades-long dietary debate, particularly about fat. The basis for promoting a lowfat diet for the treatment of heart disease was the idea that the plaque in the arteries was from fat that somehow congealed in the arter- ies. From that perspective, eating a lowfat diet would either prevent heart disease from hap-
pening in the first place or possibly reverse it if you already had it. Even in alternative medicine, there really were no other explanations put forth about heart disease, other than the debate about whether to eat a high- fat/low-carbohydrate or a lowfat diet. The only other treatment option that anybody suggested was chelation therapy, which is based on the idea that putting chelating agents into the blood- stream would somehow eat up or dissolve plaque.
Everyone agrees that there is something in the blood that is forming
plaque, and they try to reduce that “something in the blood” through diet or statin drugs. Ev- eryone also recognizes that the blood that goes through the coronary arteries is the same kind of blood as the blood that goes through the splenic artery that leads to the spleen or through any other artery. Thus, plaque formation occurs not just in our coronary arteries but also in the splenic artery, the femoral artery, the hepatic artery and so forth. Yet while all of us know someone who has had a heart attack, how many people know someone who has had a “spleen attack?” Nobody. I was an emergency room (ER) doctor for ten years, and I never once saw
Wise Traditions
SUMMER 2017
