





As the population of the industrialized world ages, illnesses associated with aging consume a larger portion of our healthcare budgets and impose increasing burdens on the quality of life of patients and their caregivers. Estimates suggest that in the U.S., Alzheimer’s disease (AD) affects 12 percent of people over age 65 and nearly 50 percent of those over 85, with predictions for this to include 16 million people by 2050.1 National healthcare costs associated with AD are expected to surpass one trillion dollars by mid-century.1
Considering the fact that AD has no known cure and current therapies are largely ineffective, identifying the triggering mechanisms and exacerbating factors behind AD is of paramount importance, as prevention and early detection would serve to decrease—or at the very least delay—the physical, emotional and financial hardships this illness creates. Prevention is also critical because AD symptoms often do not appear until loss of functional neurons is so widespread that irreversible damage has already occurred.
Significant epidemiological and clinical evidence has emerged that suggests AD belongs among the “diseases of civilization,” primarily caused by modern Western diets and lifestyles at odds with human physiology. High intakes of refined carbohydrates and omega-6-rich polyunsaturated oils, low antioxidant intake, lack of physical activity, and misguided avoidance of cholesterol and saturated fats combine to create a perfect storm for glycation and oxidative stress in the brain, ultimately resulting in severe cognitive decline that renders nearly impossible the tasks involved in everyday living.
Our evolutionarily discordant dietary environment has been linked to conditions as diverse as heart disease, diabetes, rheumatoid arthritis, polycystic ovarian syndrome (PCOS), and schizophrenia.2,3 Often, the brain is seen as a space unto itself, as though the blood-brain barrier were an impenetrable border that spares the brain the deleterious effects the rest of the body suffers as a result of a physiologically incongruous diet. However, research on AD confirms that not only is the brain as susceptible to metabolic and environmental insults as the rest of the body, but due to its high energy demands, disproportionate oxygen consumption, high concentration of oxidation-prone long-chain polyunsaturated fatty acids (PUFAs), and decreased capacity for regeneration, the brain is especially vulnerable to the detrimental effects of modern Western diets.2-10
Research into AD pathology, like that of many of its chronic, degenerative illness counterparts, is riddled with uncertainty regarding which factors are causative and which are merely correlative. Nevertheless, up-to-date literature points to genetic and environmental factors that greatly increase the risk for developing this condition. The risk profile has a strong basis in epigenetics—the influence of diet and lifestyle on how particular genotypes are expressed. The two most striking risk factors appear to be hyperinsulinism and possession of one or two E4 alleles for the apolipoprotein E gene (ApoE4), which is involved in lipid processing. (See sidebar on page 34.)
Possession of an E4 allele is so strongly correlated with AD that one study author calls it the “susceptibility gene.”11 ApoE4 heterozygotes (people with one allele) have a five-fold increased risk of developing AD, and homozygotes (two alleles) are estimated to have a staggering lifetime risk between 50-90 percent.12 Despite this seemingly damning genetic heritage, the ApoE4 allele is neither required nor sufficient for development of AD, as 50 percent of people with AD are not carriers, and some E4 homozygotes never develop the disease.13 On the other hand, the other known risk factor—hyperinsulinism—elevates risk by 43 percent independently of ApoE status. As hyperinsulinemia occurs in approximately 40 percent of people over age sixty, it’s not surprising that it correlates with a condition that preferentially strikes the aging.14
Some researchers believe the connection between impaired glucose metabolism, insulin signaling and AD is so strong that they refer to AD as “type 3 diabetes.”15 In fact, type 2 diabetes (T2D)—a condition stemming from broken glucose metabolism and insulin signaling—has been identified as an additional risk factor for developing AD.16,17 Moreover, the pathological changes that occur in AD in the brain physically resemble those seen in the pancreas and vasculature in T2D.9,18 Type 2 diabetics who carry ApoE4 alleles are at the greatest risk for AD, with an even more severe risk reserved for those treated with exogenous insulin.19 This suggests that either T2D or related features of the metabolic syndrome bring about AD, or that they are separate consequences of the same underlying cause—and moreover, that insulin is a key factor.
That not all type 2 diabetics develop AD and not all AD patients are diabetic should disabuse us of the notion that diabetes causes AD. What is more likely—and what the research seems to support—is that they are physiological cousins. That is, they result from the same underlying metabolic imbalances, but manifest differently depending on which parts of the body are affected.
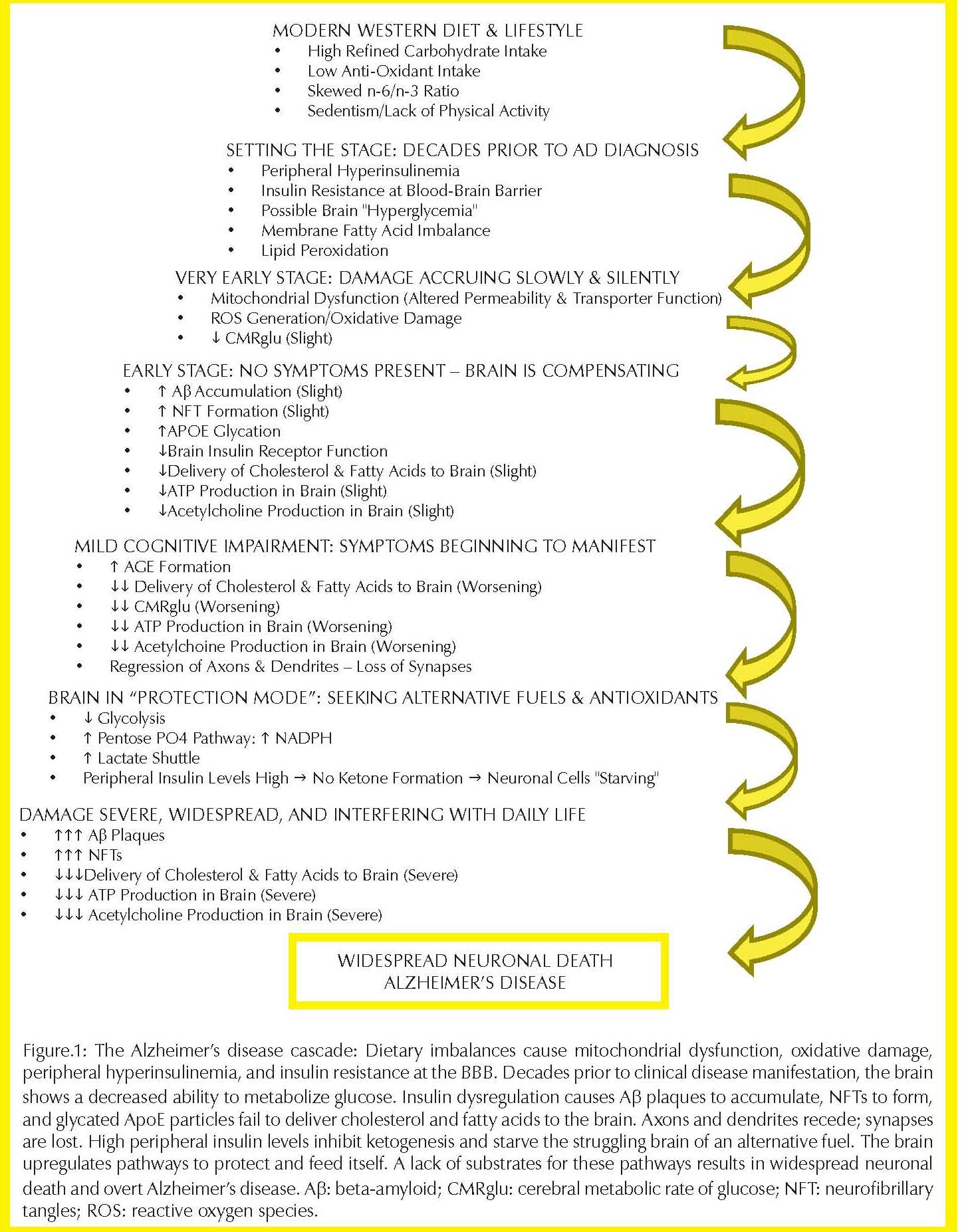
Clinically, AD patients have decreased cognitive function and lapses in memory that decline progressively and ultimately affect performance of tasks involved in everyday living. Physiologically, AD is characterized by several physical hallmarks that can be measured or observed via biopsy, positron emission tomography (PET) scan, or upon autopsy. These include insoluble extracellular plaques made of beta-amyloid peptide (Aβ); intracellular neurofibrillary tangles (NFTs) resulting from the hyperphosphorylation of tau (a microtubule-associated protein); loss of hippocampal neurons; a decrease in production of brain acetylcholine; and a marked decline in glucose usage in regions of the brain associated with memory and learning.5,11,20-22 All of these changes can be logically explained as the sequelae resulting from long-term dysregulation of insulin signaling and glucose metabolism. Their damaging effects are compounded by other features of a modern Western diet and lifestyle apart from an evolutionarily discordant degree of refined carbohydrate consumption—namely, a gross imbalance between n-6 and n-3 essential fatty acids, a lack of micronutrient and antioxidant- rich vegetables and fruits, and a paucity of physical activity.
PHYSICAL HALLMARKS OF AD: REDUCTION IN CEREBRAL USAGE OF GLUCOSE
One of the most striking observations in AD patients is a marked decline in the rate at which their brains use glucose (called the cerebral metabolic rate of glucose [CMRglu]). Specifically, this reduced fuel usage is localized in regions of the brain involved in memory processing and learning.10,11,21,24 PET scans of people at high risk for developing AD show that this decline occurs long before symptoms of AD are present, and seems to be the first step in a long chain of events whose eventual end is overt AD. The decline can be detected in those at risk as young as their twenties and thirties—decades before the manifestation of AD.11 More dramatic declines are seen in later years, with the largest declines occurring in ApoE4 homozygotes.20 These declines are associated with normal aging, but in people at risk for AD, they begin at a younger age and decline more aggressively.
It is noteworthy that the subjects tested in younger years are cognitively normal; they show no clinical signs of AD, so there is little reason to suspect that metabolic and cognitive derangement are brewing. This slow decline in brain glucose usage can be seen as a kind of “canary in the coal mine”—preclinical evidence that something has gone awry long before damage has progressed to the point of overt signs and symptoms. With the brain’s disproportionate consumption of fuel (at just 2 percent of body weight, it uses around 20 percent of the body’s glucose and oxygen), any regional reduction in fuel metabolism will have dramatic effects.25
The extent of the reduction in CMRglu is tied to AD severity. A longitudinal study using PET scans to measure CMRglu in people ages fifty to eighty showed that people with the lowest CMRglu at baseline experienced the quickest development of overt AD.24 At baseline, hippocampal glucose metabolism in people who progressed from normal to AD was 26 percent below that of people who did not develop AD, and the annual rate of decline averaged 4.4 percent. Assuming the rates of decline were somewhat constant, extrapolating backward indicates that the decline may have started several years before baseline testing, and possibly decades before any overt signs of AD were present. At baseline, despite the already decreased CMRglu in some subjects, all subjects were cognitively normal. This suggests that reduced glucose utilization in the brain might be one of the earliest events in AD. The occasional foibles and forgetfulness we associate with normal aging could, in fact, be the earliest signs that the brain is losing its ability to fuel itself effectively.
NEUROFIBRILLARY TANGLES
A second physical hallmark of AD is intracellular neurofibrillary tangles (NFTs) made of hyperphosphorylated tau protein. Tau is a protein that binds to microtubules and promotes stabilization of the cell’s internal structure. Hyperphosphorylated tau does not bind to microtubules and instead tangles in upon itself, leaving this debris inside the cell, and also resulting in an improperly constructed cytoskeleton, leading to compromised cell function.12,26 A critical result of malformed microtubules is loss of structure and function in neuronal axons and dendrites—the projections responsible for cellular communication— sending and receiving electrical impulses and metabolic materials.26
What, then, causes the phosphorylation of tau? This is regulated by the enzyme glycogen synthase kinase 3β (GSK-3β). Insulin inhibits this enzyme, so if the brain is insulin resistant, the process is not inhibited. An interesting feature ties hyperphosphorylated tau back to ApoE4. Of the three isoforms of ApoE, E4 is unique in its inability to bind tau. The E3 isoform has been proven to bind to tau (with the same suspected for E2), thus preventing or minimizing its phosphorylation.
BETA-AMYLOID PEPTIDE
The most prominent physical characteristic of an AD brain is the accumulation of insoluble extracellular plaques consisting of beta-amyloid peptide (Aβ). Aβ results from the normal cleavage of amyloid precursor protein (APP), but its accumulation and aggregation into plaques represents the quintessential feature of AD.27 Aβ is found in orders of magnitude greater in AD brains than in healthy brains.28 This fact is noteworthy because lower concentrations of Aβ tend to stay soluble; higher concentrations form plaques more readily.29
If these plaques are either causing or exacerbating AD, it is crucial to identify why they’re being secreted out of the cell and why they are not degraded normally. It has been shown that insulin is behind both of these phenomena: insulin stimulates the secretion of the two forms of Aβ associated with AD, and it also inhibits its degradation and clearance.30
Rather than increased production of Aβ inside the cell, research indicates that reduced extracellular clearance is what causes Aβ to accumulate. Aβ is cleared primarily by insulin degrading enzyme (IDE). The affinity of IDE for insulin is so high, however, that the presence of even small amounts of insulin completely inhibits the degradation of Aβ.30 Insulin acts as a kind of competitive inhibitor, such that when insulin is present, IDE will be “busy” clearing it, leaving Aβ to accumulate. Hyperinsulinemia equates to a functional (if not clinical) “IDE deficiency.” This strikes an even bigger blow to aging populations because IDE production declines with age, so there is an increasing amount of substrate combined with lower enzyme activity.31
Just as insulin can be seen as a competitive inhibitor of IDE for degradation of Aβ, Aβ can be viewed as a competitive inhibitor of insulin for its receptor. This has been proven in human cells in vitro—Aβ reduces the binding of insulin to its receptor in a dose-dependent manner.28 Insulin levels are already reduced in the brain of AD patients, and now there is something interfering with the proper binding of what little insulin is present.
Due to reduced clearance via IDE, Aβ accumulates, and the more it accumulates, the more prone it is to form insoluble plaques. Two other factors contributing to plaque formation are intimately related to the genetic and metabolic risk factors for AD—ApoE genotype and hyperinsulinism (with attendant hyperglycemia). Autopsy of human AD brains shows that the amount of plaque present and its density are directly influenced by ApoE genotype, with E4 homozygotes having the densest and most extensive plaques. Sections from the brains of homozygous ApoE4 AD patients are so riddled with Aβ plaques that they can often be distinguished from those of E3 carriers without a microscope.32
ApoE particles themselves have been identified in amyloid plaques. However, strong evidence that they bind directly to the plaques is lacking. What has been established is the fact that ApoE particles bind to advanced glycation end products (AGEs), and yet another factor contributing to the insolubility of the plaques is their degree of glycation. The plaques become glycated (bonded to sugar) and form cross-linkages with each other, resulting in toxic AGEs. It is the glycated plaques and AGEs that the ApoE particles actually bind to. Glycation is a factor of glucose concentration exposure and time, with more AGEs forming upon longer exposure to higher concentrations of glucose.33 It follows that in a body that is hyperinsulinemic, and a brain that is insulin-resistant, the peripheral hyperinsulinism will inhibit the clearance of soluble Aβ by IDE, thereby causing it to remain in the extracellular space for an extended amount of time, and the functional “hyperglycemia” in the brain will provide an elevated level of glucose—the perfect storm for glycation of Aβ and its aggregation into insoluble plaques. As if that were not challenge enough for a brain that is already struggling to metabolize fuel efficiently, AGEs themselves have been shown to be neurotoxic, likely by inducing apoptosis (cell death) and lipid peroxidation—a process that is especially damaging to cells whose membranes are particularly rich in PUFAs.10,33
Similar to the reduction in the CMRglu, AGE accumulation is a normal product of aging, but AGE formation occurs more quickly and to a greater degree in AD patients. AD brains show more AGEs than those of healthy, age-matched controls.34 ApoE4 particles have been shown to have three times greater AGE-binding affinity than ApoE3, and apolipoprotein particles themselves are subject to glycation. Increased glycated ApoE particles have been detected in the cerebrospinal fluid (CSF) of AD patients.34,35 The physiological insult of glycated ApoE is that ApoE helps transport LDL particles (and their critical cholesterol and fatty acid passengers) across the blood brain barrier. LDL containing normal ApoE will be recognized by its receptor and proceed through, while glycated ApoE is not recognized, thus depriving brain cells of these essential building blocks.6
There is even more to the interaction of ApoE genotype and Aβ. ApoE genotype influences insulin degrading enzyme production, with E4 homozygotes expressing 50 percent less hippocampal IDE than non-E4 carriers.27 It is not known whether the ApoE4 genotype causes reduced IDE. They could both arguably be the result of an overall hunter-gatherer genotype not designed for the carbohydrate-rich Western diet. Pre-agriculturalists presumably would have derived more of their calories from fat and protein and would therefore have had a lower requirement for both insulin and IDE.36,37
Several authors have asserted that Aβ is toxic. Aβ is believed to penetrate neuronal plasma membranes, where it leads to lipid peroxidation.10 It has also been implicated in deactivating a subunit of the pyruvate dehydrogenase complex, thereby inhibiting conversion of pyruvate to acetyl CoA and the eventual production of cellular energy as ATP.32 Another way Aβ affects glucose metabolism in the brain is that fragments of Aβ disrupt insulin signaling by binding to neuronal synapses, which alters their shape and function.15,38 Insulin receptors are abundant at synapses, so if the integrity of the synapse itself has been compromised, the receptors won’t function effectively.
It’s easy to see why one school of thought subscribes to the belief that Aβ plaques cause AD. However, an alternative theory is emerging wherein Aβ is argued to be protective. This more holistic view of AD pathology will be addressed after a discussion of the critical role of insulin in AD causation and progression.
INSULIN’S ROLE IN AD PATHOLOGY
It had long been believed that glucose uptake in the brain was entirely independent of insulin, as the common brain glucose transporters— GLUT1 and GLUT3—are non-insulin-sensitive. However, it is now recognized that there are insulin receptors and insulin-sensitive glucose transporters (GLUT4) at the blood brain barrier (BBB) and in certain brain cells. They are particularly abundant in regions involved in memory and learning.39,40
Entry of insulin into the brain is a saturable mechanism; there comes a point when increased peripheral insulin levels no longer elevate levels in the central nervous system (CNS). Entry of glucose into the brain can be seen as saturable as well. GLUT1 transporters at the BBB are saturated by normal physiological concentrations of glucose.41 Therefore, increasing glucose uptake by the brain would require an upregulation of insulin receptors or GLUT4s. But when the receptors have been compromised, it could equate to a functional hypoglycemia in the brain, which would account for the decreasing rate of brain glucose metabolism that is one of the defining features of AD. On the other hand, if a physiologically normal amount of glucose is entering the brain interstitial fluid but there’s a lack of insulin, this could result in the increased glycation observed in AD brains. The presence of glucose with an inability to metabolize it would account for both the reduced CMRglu and increased AGE formation.
A noteworthy feature of AD is the intriguing combination of hyperinsulinism (too much) in the periphery and hypoinsulinism (not enough) in the CNS. Patients with advanced AD show higher plasma but lower CSF insulin concentrations than healthy controls.40 Clearly, then, the lower concentration of insulin in the brain is not a result of reduced circulating levels in the blood. Somehow—partly through the effects of Aβ, but more likely due to long-term overconsumption of refined carbohydrates—the brain becomes insulin-resistant.
Insulin plays a definite role in cognitive function. However, as is true of most biological mechanisms, context must be taken into account: acute administration of insulin improves performance on tests of memory and cognition, but chronically elevated insulin levels have the opposite effect.4,42,43 This is akin to the pathology of T2D, in which normal, acute doses of insulin help regulate glucose uptake, but chronically elevated levels lead to insulin resistance, hyperglycemia, and the attendant inflammation and vascular damage. Chronically elevated insulin levels in the periphery, it seems, depress insulin sensitivity at the BBB and therefore glucose utilization in the brain. In the absence of an alternative fuel source, brain cells starve. Metabolic fuel is inside the body, but the brain cells are not able to harness energy from it. The parallels to T2D are striking, making the term “type 3 diabetes” apropos.
For non-ApoE4 carriers, diabetes alone is a significant risk factor for AD.17 The combination of diabetes and carrying an ApoE4 allele increases the risk even further—five-fold over non-diabetic, non-E4 carriers.16,17,19 Better glycemic control has been correlated to better cognitive performance in type 2 diabetics. Moreover, these same subjects had improved performance on memory tests quickly after an acute dose of 50g of easily digestible carbohydrate, but this was followed by decreased performance after an extended waiting period, reflecting the aforementioned observations of acute versus chronically elevated insulin levels and glucose utilization.44 The question, then, is whether diabetes plays a causal role in AD. Research does not support this, as not all AD patients are diabetic, and not all diabetics develop AD. Due to the overwhelming evidence of insulin and glucose signaling derangement as the strongest factors in AD, it seems more likely that T2D and AD are different manifestations of the same underlying causes: in T2D, the peripheral muscles and organs are affected; in AD damage is localized to the brain.
DISCUSSION
Like that of many of its complex neurodegenerative counterparts, AD research is stymied by the problem of identifying what the first steps are in a vicious cycle wherein an underlying disturbance is perpetuated by the very results of the disturbance. The physiological and biochemical changes observed in AD point to a brain that is struggling to maintain its viability. It downregulates the uptake of glucose, upregulates mechanisms to use alternative fuels, and increases production of protective substances.
Many researchers see the accumulation of Aβ as the triggering event in AD pathology. However, a more integrated view of the innate wisdom of the human body suggests that Aβ initially serves a protective role, just as a fever is a protective mechanism rather than something to be annihilated unquestioningly. Nevertheless, just as a fever spiking too high can create problems of its own, increasing numbers and density of Aβ plaques in a hyperglycemic brain can initiate chain reactions of glycation and oxidation that serve to exacerbate mitochondrial dysfunction, decreased ATP production, and cognitive decline.
It is unlikely that Aβ plaques are a primary causative factor in AD because the effects of reduced glucose uptake in the brain are observed long before the plaques are evident. The plaques more logically result from functional inhibition of IDE due to peripheral hyperinsulinemia. Some progressive researchers have suggested that insulin resistance at the BBB is the brain’s way of forcing a slowdown in the metabolism of glucose. This seems illogical if glucose is the brain’s primary fuel (assuming a carbohydrate-rich diet). Why would the brain seek to limit the uptake of its main fuel? Several mechanisms are at work, and they all indicate that the brain is protecting its own survival while trying to minimize further damage.
First, high levels of glucose in brain interstitial fluid are glycating. Glycated proteins and cellular structures have altered function, increased vulnerability to oxidative damage, and reduced degradation and clearance.6 Slowing the entry of glucose into the brain would delay these processes and possibly give the body’s defenses more time to dispose of the AGEs.
Second, glucose metabolism causes a heavy burden of oxidative stress. The running of the mitochondrial electron transport system (ETS) is the greatest source of reactive oxygen species (ROS) and free radicals in the body, and neurons are particularly susceptible to oxidative stress because their metabolic rate is higher than that of other brain cells.10 Moreover, neuronal membranes are rich in long-chain PUFAs and cholesterol, which are highly vulnerable to oxidation. 22 AGEs have been shown to induce lipid peroxidation, so exposure of fragile membrane PUFAs to a hyperglycemic environment can be considered toxic. In an organ that is potentially so highly damaged from a lifetime of dietary and environmental abuse, downregulating the usage of a fuel whose metabolism creates even more damage can be seen as a last-ditch effort just to survive.
Third, the brain could be redirecting its metabolic machinery toward utilization of fuels other than glucose, such as fatty acids and ketone bodies, which produce less oxidative stress and are, in fact, more efficient fuels.14,46,47
One way in which Aβ serves a potentially helpful role is that it upregulates production of amyloid-β-peptide-binding alcohol dehydrogenase, an enzyme capable of metabolizing alternative fuels such as ketone bodies and alcohols.6 Another possibly protective role for Aβ is in catalyzing the production of lactate dehydrogenase, which converts pyruvate to lactate under anaerobic conditions.6 Lactate is produced in glial cells and sent to neurons, where it is converted back to pyruvate and sent through the tricarboxylic acid (TCA) cycle to produce ATP. Up-regulating lactate production compartmentalized within the brain could be the struggling brain’s way of providing a fuel substrate when glucose usage in the brain has been compromised. Here again we have two scenarios in which Aβ seems to be priming the brain to move away from glucose.
LOW CARBOHYDRATE DIETS FOR AD THERAPY
If AD is primarily the result of a brain unable to metabolize glucose properly, then interventions aimed at preventing or improving this condition should include a transition to a fuel source other than glucose, reducing peripheral insulin levels to restore sensitivity at the BBB, and providing an abundant supply of protective substances. As a model to guide therapy, we can look to what happens during fasting, starvation, or carbohydrate restriction to see the processes by which a glucose-deprived body sustains itself. The major switch that occurs in the absence or reduction of exogenous glucose is that the body transitions to running on fatty acids, ketone bodies (KBs), and small amounts of glucose derived from gluconeogenesis (making glucose from amino acids and other substances).48,49
It is often claimed that glucose is the brain’s only fuel, or that the brain requires upwards of 120 grams of glucose per day. This grossly oversimplifies human physiology. Glucose is regularly cited as the “preferred” fuel for the body and brain. However, it is only preferred in the sense that it will generally be used first. It is neither more efficient nor safer than two of the other fuels the body and brain can run on: fatty acids and KBs. KBs can provide up to 60 percent of the brain’s energy, thus sparing what little glucose is metabolized to supply the rest.47
KBs are often viewed as toxic, but this is not the case. They are an absolutely normal part of human energy metabolism that preferentially fuel the brain while much of the rest of the body runs on fatty acids during times of carbohydrate unavailability.50 The negative view of KBs stems from confusion of benign dietary ketosis (BDK) and diabetic ketoacidosis (DKA). BDK occurs as a result of dramatic reductions in carbohydrate consumption, while DKA is seen in untreated type 1 diabetics, who do not produce insulin, have extremely limited capacity to burn glucose, and therefore are in a constant, uncontrolled state of catabolizing (breaking down) their own muscle and adipose tissue to use as fuel. Despite both conditions indicating that the body is burning fat at a high rate, they are worlds apart in physiological implication. During BDK from carbohydrate reduction, blood ketone concentrations are typically no higher than 4-6 mM, with no change in blood acidity. In DKA, however, blood ketone concentration can reach up to 25 mM—orders of magnitude greater—and blood pH can decrease to fatal levels that overwhelm the body’s acid buffering capacity.47
Ketogenic diets have a long history of efficacy for disorders of the CNS, most notably epilepsy.46,47 KBs are more efficient than glucose and induce less oxidative damage.47 Additionally, KBs are brought into the brain by monocarboxylate transporters—independently of glucose and insulin—so their uptake is not hindered when insulin signaling fails.51
This raises the question, if the brain is struggling to use glucose, why does it not immediately shift to fueling with ketones? The answer is that sufficient ketones aren’t available. Due to differing requirements of various tissue systems, the body as a whole runs on glucose, fatty acids, and KBs concurrently to some extent. However, the pathways are largely antagonistic; where one predominates, another is inhibited. Glucose induces insulin secretion, and insulin inhibits CPT-1, an enzyme responsible for bringing fatty acids into the mitochondria to be used. Therefore, when insulin levels are high, fatty acids are not well used as fuel and no significant ketogenesis occurs. (KBs are a byproduct of fatty acid metabolism.) So even though the brain is starving for fuel, KBs will not be produced in sufficient quantity. The end result for an AD patient is that the brain is not metabolizing glucose effectively and no alternative fuels are available. For neuronal cells that have such enormous energy requirements, the consequences of this disruption in fuel supply are devastating.
If ketones are the brain’s primary fuel source under conditions of reduced glucose availability, then AD patients should show improvements in cognitive function on a ketogenic diet or with administration of exogenous ketones. This has been demonstrated in randomized, double-blind, placebo-controlled studies. In two studies, oral administration of KBs via medium-chain triglyceride (MCT) drink mixes resulted in improved performance on cognition tests compared to placebo, and this was achieved even in the absence of dietary carbohydrate reduction.
In a study involving dietary ketosis via a low carbohydrate diet (less than 10 percent of total calories), compared to subjects on a 50 percent carbohydrate diet, the low-carbohydrate subjects demonstrated better performance on memory tests, with higher scores being correlated to higher serum KB levels.14 A study using cultured mouse hippocampal cells showed that addition of the KB β-hydroxybutyrate (β-OHB) to cells exposed to Aβ resulted in no decrease in the numbers of dendrites or total neurons—two of the noted pathological changes in AD. Addition of β-OHB at a 4 mM concentration—achievable on a very low carbohydrate diet—doubled the surviving number of cells and actually increased dendritic growth.52 Analyses of brains of people who have aged free of cognitive decline have shown that a loss of neurons can be compensated for by an increase in dendrites of the remaining neurons so there is no net loss of synapses.49
If the primary metabolic change that occurs during fasting or a ketogenic diet is a wholesale shift away from glucose and toward fatty acids and ketones for fuel, with the resultant lowering of blood glucose and insulin levels and restoration of insulin sensitivity, then reduced carbohydrate consumption should lead to similar neuroprotective effects. Moreover, if AD stems from a diet and lifestyle at odds with what our evolutionary history has prepared us for, then an abandonment of refined and chemically altered foods and a return to a more “primitive”-type diet would also likely be protective. Specifically, if the initial pathogenesis of AD comes from peripheral hyperinsulinemia, there is reason to believe that restriction of dietary carbohydrates should be frontline therapy for AD. The therapeutic and neuroprotective effects of ketone bodies are so effective, in fact, that one researcher suggests a drawback of the modern, carbohydrate-heavy diet is that it is “keto-deficient.”53
A classical ketogenic diet—with a staggering 70-90 percent of total calories coming from fat—might not be necessary.51 Classical ketogenic diets restrict protein as well as carbohydrate, since 48-58 percent of the amino acids in dietary proteins can be glucogenic, thereby undermining the purpose of a diet intended to generate a high amount of ketones and limit glucose as much as possible.46 As therapy for AD, however, simply lowering carbohydrate intake to a point where some ketones are generated and hyperinsulinemia is corrected could have positive effects just by easing the metabolic burden on the brain. That is, one could reap the “benefits” of fasting (enhanced insulin sensitivity, reduced oxidative stress, reduced AGE formation) by simply reducing carbohydrate intake to prevent chronic systemic hyperglycemia. Moreover, a ketone-producing, lower-carbohydrate diet would still allow for consumption of a wide array of low glycemic load vegetables and fruits, which are typically richer in micronutrients, antioxidants, and phytochemicals than their high glycemic load refined grain and sugar counterparts.54 This would make this primary avenue for therapy more practical, since the difficulty with sticking to classical ketogenic diets is typically that they’re unpalatable and too restrictive. This is also likely why much of the research involving KBs as AD therapy is limited to exogenous ketones and MCT preparations; classical ketogenic diets are extremely challenging to maintain. There is also likely trepidation regarding such a high fat intake—particularly saturated fat—despite mounting evidence even in the medical mainstream that saturated fat intake is not associated with increased risk for cardiovascular disease, and that reductions in carbohydrate intake, in fact, can improve risk for heart disease.55 Promising avenues for research in dietary therapy for AD are hindered by an outdated nutritional paradigm.
FUTURE AVENUES
Although the ApoE4 genotype is strongly associated with development of AD, no genetic heritage is a death sentence. Rather, it is the mismatch between this hunter-gatherer genotype and a seemingly inexhaustible supply of inexpensive, readily obtained refined sugars and carbohydrates, that brings about AD in these populations. Similarly, no genetic heritage is a free pass. Groups with other variants of the ApoE gene are not immune to the ravages of the modern diet. Hyperinsulinemia is the strongest known risk factor in non-E4 carriers, and overcomes whatever protection their genes might provide. AD is not a disease of genetics, but one of epigenetics— the influence of diet, environment, and lifestyle on how genes are expressed.
That Alzheimer’s disease appears late in life does not mean the causative cascade is not started decades earlier. Like other “diseases of civilization,” AD builds slowly over time, often with no overt symptoms, until damage is already widespread and, in some cases, irreversible. What we consider the normal forgetfulness of older age might very well be early warnings that the brain is struggling to fuel itself. Unfortunately, in the absence of clear signs of glucose dysregulation (hypo- or hyperglycemia, obesity, etc.), people have no reason to suspect something metabolically insidious is occurring. Therefore, regular monitoring of pertinent markers—such as fasting blood glucose, fasting insulin, triglycerides, and especially HbA1c—might be the only strategy for early detection.
In cases of AD detected only after cognitive function has deteriorated to the point of interfering with daily life, drastic interventions such as ketogenic diets and supraphysiologic doses of helpful nutrients might be warranted. These are avenues ripe for exploration in future research. Lifelong reduction of risk, however, should start early and include a diet low in refined sugar and carbohydrates; rich in omega-3 fatty acids (specifically DHA) and naturally occurring, stable saturated fats; rich in antioxidants and phytonutrients from low-glycemic vegetables and fruits; emphasis on whole, unprocessed foods, and inclusion of stress reduction and muscle-building physical activity.
The plethora of evidence linking hyperinsulinemia, T2D, mitochondrial dysfunction, and glucose dysregulation—all resulting from the refined, chemically manipulated modern Western diet—to Alzheimer’s disease suggests that the time has come for a drastic reevaluation of across-the-board recommendations for entire population groups to consume low-fat and low-cholesterol diets, which are, by default, high in carbohydrates. Combined with stressful and sedentary lifestyles, and particularly when complicated by cholesterol-lowering medication, this amounts to nothing less than a blueprint for creating Alzheimer’s disease and other forms of neurological degeneration.
Sidebars
WHAT IS APOLIPOPROTEIN E?
Lipoproteins are vesicles that transport non-water-soluble substances—such as fatty acids and cholesterol—through the bloodstream. Apolipoproteins appear on the surface of lipoproteins, where they serve as ligands (recognition factors) for receptors and as cofactors in enzymatic processes.8 The gene for ApoE occurs in three isoforms, and it is theorized that their distribution is related to human evolutionary migration patterns and the historic adoption of grain-based agriculture.23 Groups with the longest exposure to grain consumption have a lower E4 frequency, suggesting that high carbohydrate intakes may have selected against E4.5
The three ApoE isoforms differ by just one amino acid, but this substitution has dramatic biochemical implications.12 These single substitutions affect tendency to become glycated, as well as determine binding affinity to enzymes and receptors, which is why the three isoforms are associated with different trends in serum LDL, VLDL, and triglyceride measurements.8
Neurons have ApoE receptors, which suggests that ApoE plays a role in the delivery and clearance of fatty acids,
cholesterol, and phospholipids to and from the brain. Delivery and recycling of cholesterol in the brain is critical because the brain contains 25 percent of the body’s total cholesterol—used as an antioxidant, electrical insulator and key structural component of plasma membranes. ApoE4 is associated with reduced LDL uptake and all the consequences that would result from an inability to deliver cholesterol and fatty acids to target cells.6 Cholesterol is an essential contributor to structure and function in the brain, and any interruption in its supply would have extreme consequences for cognitive function.
WHAT TO AVOID TO HELP PREVENT ALZHEIMER’S DISEASE
• STATIN DRUGS: Cholesterol is a vital part of the myelin sheath insulating neurons and assisting in propagation of nerve impulses; metabolites in the cholesterol biosynthesis pathway inhibited by statins are required to produce CoQ10 as well as functional GLUT4s. Cholesterol is also an integral part of plasma membranes, lending structural stability. Any pharmaceutically-induced disruption in endogenous synthesis of cholesterol—especially when combined with long-standing, population-wide recommendations to limit dietary intake—would starve the struggling brain of this absolutely critical nutrient. In fact, high cholesterol levels later in life are associated with reduced risk of dementia, and the CSF of AD patients has been shown to be lower in cholesterol than that of healthy controls.62,63 HMG CoA reductase—the target of statin therapy—is abundant in brain cells. They require a constant supply of cholesterol, and when its production is inhibited, the result is a loss of myelin as well as malformation of membranes—including those of the mitochondria.8 Compromised mitochondrial function deprives the brain of ATP. It is no surprise that decades of recommendations to reduce consumption of cholesterol and perhaps overzealous prescription of statin drugs have paralleled the rise in AD incidence.6
• PROCESSED FOODS: These present a quadruple nutritional assault upon a brain suffering the ravages of the modern diet: they are usually high in refined carbohydrate; high in rancid, easily oxidized vegetable oils; low in antioxidants; and low in vitamins and minerals.
• EXOGENOUS INSULIN: Although insulin has been shown to improve memory and cognition acutely, chronically
high insulin levels are known to impair brain function.42,64 Exogenous insulin would serve to inhibit IDE more strongly, thereby preventing the clearance of Aβ, causing it to linger in the brain interstitial fluid even longer, where it is subject to glycation and oxidation. As noted, the greatest risk for AD is reserved for ApoE4 carriers who are treated with exogenous insulin.
NUTRITIONAL THERAPIES FOR ALZHEIMER’S DISEASE
The damage observed in AD brains is complex and multifactorial. Any intervention intended to delay or possibly
reverse this damage should therefore be a multipronged strategy designed to address as many of the contributing factors as possible. The majority of these potentially helpful practices are nutritional, but two can be considered lifestyle modifications. Obviously, the foundation of what might be considered an “anti-Alzheimer’s strategy” is a reduced carbohydrate diet. Beyond that, there are numerous nutritional supplements that could be effective based on their biochemical functions:
• Chromium picolinate: Chromium is required for proper function of the insulin receptor, and has been proven to aid in glucoregulation and insulin sensitivity.58,59
• Zinc: Insulin degrading enzyme requires zinc as a cofactor.57
• High-quality cod liver oil: To balance the n-6/n-3 ratio and decrease inflammation. Generally, oils rich in n-6 fatty acids induce inflammation in the body, while n-3-rich oils stimulate anti-inflammatory pathways. The ratio of n-6 to n-3 in the modern American diet is estimated to be as high as 30:1, while our evolutionary dietary patterns suggest we are physiologically suited to a ratio closer to 3:1.36,60 Additionally, dietary imbalances of these fatty acids cause imbalances in their incorporation into cellular and organelle membranes, resulting in altered permeability and increased vulnerability to lipid peroxidation.
• Medium-chain triglycerides (MCTs): These saturated fatty acids (found mostly in coconut and palm kernel oils) are metabolized differently from others and can serve as a source of ketones even in the absence of carbohydrate restriction.61
• L-Carnitine: This amino acid is required by carnitine palmitoyltransferase-1, the enzyme responsible for shuttling fatty acids into the mitochondria, as well as other enzymes in the breakdown of fats.50 A patient on a reduced carbohydrate diet with the specific intention of ramping up fatty acid oxidation and ketogenesis could likely benefit from supplemental carnitine.
• Coenzyme Q10: CoQ10 is a vital member of the mitochondrial electron transport system (and therefore generation of ATP) and also a potent antioxidant. CoQ10 administration has been shown to reduce production of ROS by mitochondria exposed to Aβ in animal models of diabetes.18 With the AD brain struggling to produce energy and under great oxidative stress, CoQ10 could be a powerful adjunct.
• Antioxidants: In addition to increasing antioxidant-rich foods in the diet, supplemental N-acetyl-cysteine for glutathione regeneration might be helpful. (It’s noteworthy that the fruits highest in antioxidants are also lower in glycemic index and load; namely, berries.) Supplemental superoxide dismutase might also be beneficial.
• Physical activity: Physical activity induces recruitment of GLUT4s and ultimately helps maintain insulin sensitivity. Resistance training or weightlifting might prove particularly beneficial, as it would serve to increase muscle mass and potentially increase insulin sensitivity. This might be especially protective if started early in life so as to minimize the impact of sarcopenia (loss of muscle mass) as one ages.
• Stress reduction: Cortisol, the primary glucocorticoid “stress hormone,” releases glucose in response to acute stressors.25 In our hyper-stressful modern environment, our bodies almost always perceive dire threats all around us. Chronically high cortisol levels could induce hyperglycemia even in the context of a reduced carbohydrate diet.
• B12: While B12 is not necessarily required for a therapeutic diet for AD, it is important to note that memory loss and cognitive decline are insidious signs of long-term B12 deficiency. Sufficient stomach acid is required for B12 absorption, and stomach acid production naturally declines with age. Combine this with the possibility that older people are less likely to consume B12-rich foods (which can take more effort to prepare than convenient, ready-to-eat refined carbohydrates), and B12 deficiency becomes fairly common in the elderly. B12 deficiency can even be mistaken for AD, so it’s worthwhile to have B12 levels tested if AD is suspected.
THERAPEUTIC INTERVENTION FOR ALZHEIMER’S DISEASE
Current Alzheimer’s disease (AD) therapies are typically piecemeal approaches aimed at treating individual symptoms, rather than addressing the underlying causes of the disease. One drug manufacturer created a pharmaceutical drug to inhibit the enzyme that creates Aβ from the amyloid precursor protein. Phase III clinical trials had to be stopped because results were so damning against this treatment. Measures of cognition and ability to complete daily living tasks were significantly worse for patients receiving the drug than the placebo.56 Yet again, here is evidence that Aβ is not a causal factor. Production of Aβ is a normal process and there is no evidence that AD patients overproduce it.57 It becomes pathological only when—due to peripheral hyperinsulinemia—it is not degraded and cleared as it should be.
Several authors have proposed administering exogenous ketone bodies via pharmaceutical MCT preparations. While this provides the brain with an alternative fuel and has been shown to improve cognitive function, it does nothing to address the myriad other issues attendant with the metabolic derangement that is likely the root cause of AD. The cognitive decline seen in AD is not a disease in itself; it is the result of a lifetime of accumulated dietary and environmental insults, which in older age finally overwhelm the brain’s capacity to protect and heal itself. Administration of KBs would neither alleviate hyperinsulinemia nor restore insulin sensitivity at the BBB. MCTs could certainly be a powerful adjunct to a reduced carbohydrate diet, which would reset the metabolic machinery, ease oxidative stress, and reduce glycation. In the absence of dramatic dietary overhaul, however, the administration of KBs is akin to bailing water out of a leaky boat without stopping to patch the hole: you merely manage the effects while the root cause continues wreaking havoc.
REFERENCES
1. Alzheimer’s Association. Alzheimer’s facts and figures. http://www.alz.org/alzheimers_disease_facts_and_figures.asp.
2. Cordain L, Eades MR, Eades MD. Hyperinsulinemic diseases of civilization: more than just Syndrome X. Comp Biochem Physiol A Mol Integr Physiol. 2003;136(1):95-112..
3. Cordain, L. Cereal grains: humanity’s double-edged sword. World Rev Nutr Diet 1999;84:19-73.
4. Craft S and Watson GS. Insulin and neurodegenerative disease: shared and specific mechanisms. Lancet Neurol 2004;3(3):169-78.
5. Henderson S. High carbohydrate diets and Alzheimer’s disease. Med Hypotheses 2004; 62:689- 700.
6. Seneff S, Wainwright G, and Mascitelli L. Nutrition and Alzheimer’s disease: the detrimental role of a high carbohydrate diet. Eur J Intern Med 2011;22(2)134-40.
7. Kanoski S and Davidson T. Western diet consumption and cognitive impairment: Links to hippocampal dysfunction and obesity. Physiol Behav 2011;103(1):59-68.
8. Lane R and Farlow M. Lipid homeostasis and apolipoprotein E in the development and progression of Alzheimer’s disease. J Lipid Res 2005;46(5):949-68.
9. Moreira P, Santos M, Seica R, et al. Brain mitochondrial dysfunction as a link between Alzheimer’s disease and diabetes. J Neurol Sci 2007;257(1-2):206-14.
10. Mamelak M. Alzheimer’s disease, oxidative stress and gammahydroxybutyrate. Neurobiol Aging 2007;28(9):1340-60.
11. Reiman E, Kewei C, Alexander G, et al. Functional brain abnormalities in young adults at genetic risk for late-onset Alzheimer’s dementia. Proc Natl Acad Sci USA 2004;101(1):284-289.
12. Kamboh, MI. Apolipoprotein E polymorphism and susceptibility to Alzheimer’s disease. Hum Bil 1995;67:195-215.
13. Qiu W and Folstein M. Insulin, insulin-degrading enzyme and amyloid-β peptide in Alzheimer’s disease: review and hypothesis, Neuro Biol Aging 2006;27:190-198
14. Krikorian R, Shidler M, Dangelo K, et al. Dietary ketosis enhances memory in mild cognitive impairment. Neurobiology of Aging 2012;33:425e19-425e27.
15. Kroner Z. The relationship between Alzheimer’s disease and diabetes: Type 3 diabetes? Altern Med Rev. 2009;14(4):373-9.
16. Irie F, Fitzpatrick A, Lopez O, et al. Enhanced risk for Alzheimer disease in persons with type 2 diabetes and APOE ε4. Arch Neurol 2008;65(1):89-93.
17. Peila R, Rodriguez B, and Launer L. Type 2 diabetes, APOE gene, and the risk for dementia and related pathologies – the Honolulu-Asia aging study. Diabetes 2002;51:1256-1262.
18. Moreira P, Santos M, Sena C, et al. CoQ10 therapy attenuates amyloid β-peptide toxicity in brain mitochondria isolated from aged diabetic rats. Exp Neurol 2005;196(1):112-9.
19. Ott A, Stolk R, Van Harskamp F, et al. Diabetes mellitus and the risk of dementia: the Rotterdam study. Neurology 1999;53(9)1937-42.
20. Reiman E, Caselli R, Yun L, et al. Preclinical evidence of Alzheimer’s disease in persons homozygous for the e4 allele for apolipoprotein E. NEJM 1996; 334(12):752-758.
21. Fukuyama H, Ogawa M, Yamauchi H, et al. Altered cerebral energy metabolism in Alzheimer disease: a PET study. J Nucl Med 1994;35(1):1-6.
22. Correia S, Santos E, Carvalho C, et al. Insulin signaling, glucose metabolism and mitochondria: Major players in Alzheimer’s disease and diabetes interrelation. Brain Research 2012;1441:64-78.
23. Corbo RM and Scacchi R. Apolipoprotein E (APOE) allele distribution in the world. Is APOE
4 a ‘thrifty’ allele? Ann Hum Genet 1999;63(4):301-10.
24. Mosconi L, De Santi S, Li J, et al. Hippocampal hypometabolism predicts cognitive decline from normal aging. Neurobiol Aging 2008;29(5):676-692.
25. Tortora G, Derrickson B, eds. Principles of Anatomy and Physiology. Hoboken, NJ: John Wiley & Sonds, Inc., 2006;474.
26. Strittmatter W and Roses Allen. Apolipoprotein E and Alzheimer’s disease. Annu Rev Neurosci 1996;19:53-77.
27. Cook D, Leverenz J, McMillan P, et al. Reduced hippocampal insulin-degrading enzyme in late-onset Alzheimer’s disease is associated with the apolipoprotein E-ε4 allele. Am J Pathol 2003;162(1):313-9.
28. Xie L, Helmerhorst E, Taddei K, et al. Alzheimer’s β-amyloid peptides compete with insulin for binding to the insulin receptor. J Neurosci. 2002;22(10):RC221.
29. Qiu W, Walsh D, Ye Z, et al. Insulin-degrading enzyme regulates extracellular levels of amyloid β-protein by degradation. J Biol Chem 1998;273(49):32730-8.
30. Gasparini L, Gouras GK, Wang R, et al. Stimulation of beta-amyloid precursor protein trafficking by insulin reduces intraneuronal beta-amyloid and requires mitogen-activated protein kinase signaling. J Neurosci 2001;21(8):2561-70.
31. Hoshi M, Takashima A, Noguchi K, et al. Regulation of mitochondrial pyruvate dehydrogenase activity by tau protein kinase I/glycogen synthase kinase 3beta in brain. Proc Natl Acad Sci USA 1996;93(7):2719-23.
32. Schmechel DE, Saunders AM, Strittmatter WJ, et al. Increased amyloid β-peptide deposition in cerebral cortex as a consequence of apolipoprotein E genotype in late-onset Alzheimer disease. Proc Natl Acad Sci USA 1993;90:9649-53.
33. Takeuchi M, Sato T, Takino J, et al. Diagnostic utility of serum or cerebrospinal fluid levels of toxic advanced glycation end-products (TAGE) in early detection of Alzheimer’s disease. Med Hypotheses 2007;69(9)1358-66.
34. Li Y and Dickson D. Enhanced binding of advanced glycation endproducts (AGE) by the ApoE4 isoform links the mechanism of plaque deposition in Alzheimer’s disease. Neur Letters 1997;26:155-158.
35. Shuvaev VV, Laffont I, Serot JM, et al. Increased protein glycation in cerebrospinal fluid of Alzheimer’s disease. Neurobiol Aging 2001;22(3):397-402.
36. Cordain, L Eaton SB, Sebastian A, et al. Origins and evolution of the Western diet: health implications for the 21st century. Am J Clin Nutr 2005;81:341-354.
37. Cordain L Eaton SB. Evolutionary aspects of diet: old genes, new fuels. World Rev Nutr Diet 1997;81:26-37
38. Viola KL, Velasco PT, Klein WL. Why Alzheimer’s is a disease of memory: the attack on synapses by A beta oligomers (ADDLs). J Nutr Health Aging 2008;12(1):51S-7S.
39. Woods S, Seeley R, Baskin D, et al. Insulin and the blood-brain barrier. Curr Pharm Des 2003;9(10):795-800.
40. Craft S, Peskind E, Schwartz M, et al. Cerebrospinal fluid and plasma insulin levels in Alzheimer’s disease – relationship to severity of dementia and apolipoprotein E genotype. Neurology 1998;50:164-168.
41. Convit, A. Links between cognitive impairment in insulin resistance: an explanatory model. Neurobiol Aging 2005;26 Suppl 1:31-5.
42. Watson G, Peskind E, Asthana S, et al. Insulin increases CSF Aβ42 levels in normal older adults. Neurology 2003;60(12):1899-903.
43. Luchsinger J, Tang M-X, Shea S, et al. Hyperinsulinemia and risk of Alzheimer’s disease. Neurology 2004;63:1187-1192.
44. Greenwood CE, Kaplan RJ, Hebblethwaite S, et al. Carbohydrate-induced memory impairment in adults with type 2 diabetes. Diabetes Care 2003;26(7):1961-6.
45. Schubert D. Glucose metabolism and Alzheimer’s disease. Ageing Res Rev 2005;4(2):240-57.
46. VanItallie T and Nufert T. Ketones: metabolism’s ugly duckling. Nutr Rev 2003;61(10):327-41.
47. Veech R. The therapeutic implications of ketone bodies: the effects of ketone bodies in pathological conditions: ketosis, ketogenic diet, redox states, insulin resistance, and mitochondrial metabolism. Prostaglandins Leukot Essent Fatty Acids 2003;70(3):309-19.
48. Martin B, Mattson MP, Maudsley S. Caloric restriction and intermittent fasting: two potential diets for successful brain aging. Ageing Res Rev 2006;5(3):332-53.
49. Prolla TA, Mattson MP. Molecular mechanisms of brain aging and neurodegenerative disorders: Lessons from dietary restriction. Trends Neurosci 2001;24(11 Suppl):S21-31.
50. Devlin T, ed. Textbook of Biochemistry with Clinical Correlations. Hoboken, NJ:John Wiley & Sons, Inc., 2011;691-702.
51. Gasior M, Rogawski M, and Hartman A. Neuroprotective and disease-modifying effects of the ketogenic diet. Behav Pharmacol 2006;17(5-6):431-9.
52. Kashiwaya Y, Takeshima T, Mori N, et al. D-β-Hydroxybutyrate protects neurons in models of Alzheimer’s and Parkinson’s disease. Proc Natl Acad Sci USA 2000;97(10):5440-4. 53. Henderson S. Ketone bodies as a therapeutic for Alzheimer’s disease. Neurotherapeutics 2008;5(3):470-80.
54. Cordain L. The nutritional characteristics of a contemporary diet based on Paleolithic food groups. J Am Nutraceut Assoc 2002;5:15-24.
55. Siri-Tarino P, Sun Q, Hu F, et al. Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. Am J Clin Nutr 2010;91(3):535-46.
56. Eli Lilly and Company. Lilly Halts Development of Semagacestat for Alzheimer’s Disease Based on Preliminary Results of Phase III Clinical Trials. Aug 17, 2010. http://newsroom.lilly.com/releasedetail.cfm?releaseid=499794.
57. Miller B, Eckman E, Sambamurti K, et al. Amyloid-β peptide levels in brain are inversely correlated with insulysin activity levels in vivo. Proc Natl Acad Sci USA 2003;100(10)6221-6.
58. Lamson DW, Plaza SM. The safety and efficacy of high-dose chromium. Altern Med Rev 2002;7(3):218-35.
59. Cefalu WT, Rood J, Pinsonat P, et al. Characterization of the metabolic and physiologic response to chromium supplementation in subjects with type 2 diabetes mellitus. Metabolism 2010;59(5):755-62.
60. Denniston K, Topping J, Caret R. General, Organic, and Biochemistry. New York, NY;McGraw- Hill, 2011;574 and 772-773.
61. Henderson ST, Vogel JL, Barr LJ, et al. Study of the ketogenic agent AC-1202 in mild to moderate Alzheimer’s disease: a randomized, double-blind, placebo-controlled, multicenter trial. Nutr Metab (Lond) 2009;6:31.
62. Mielke MM, Zandi PP, Sjögren M, et al. High total cholesterol levels in late life associated with a reduced risk of dementia. Neurology 2005;64(10):1689-95.
63. Mulder M, Ravid R, Swaab DF, et al. Reduced levels of cholesterol, phospholipids, and fatty acids in cerebrospinal fluid of Alzheimer disease patients are not related to apolipoprotein E4. Alzheimer Dis Assoc Disord 1998;12(3):198-203.
64. Reger MA, Watson GS, Green PS, et al. Intranasal insulin administration dose-dependently modulates verbal memory and plasma amyloid-β in memory-impaired older adults. J Alzheimer’s Dis 2008;13(3):323-31.
This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly journal of the Weston A. Price Foundation, Summer 2014
🖨️ Print post
A copy of this paper should be hand delivered to every member of Big Pharma. You can stop looking for a “CURE;” we have one- involving real food and lifestyle modifications. I’m betting my ApoE4/4 life on it. Congrats, Amy, on a seminal paper. Excellent job connecting the multifactorial processes behind this devastating disease.
Thanks, Julie! I agree — I wish every gerontologist and neurologist would stumble upon this… In my opinion, AD is entirely preventable, and if not *completely* reversible once it’s created a lot of damage, then at the very least we can stop further damage from accruing and possibly even, over time, undo *some* of the long-term effects. It’s criminal that people continue to lose their life savings and their lives to this condition when there is absolutely something we can do about it — something that doesn’t involve thousands of dollars’ worth of ineffective drugs and long-term care.
Amy, impressive research, as a sixty something I’m taking heed of your research plus sending this to my kids. Thank you!
Anne
Great article. Have shared and posted it far and wide amongst friends, nutritionist and herbalists.
Thank you! This is a beacon of hope to all of us who have been touched by AD. Even though other authors make the very low carb/ketogenic diet recommendation (Mercola), your research presents it most convincingly. Many, many thanks!
Thanks, Frank! Glad you’ve found something useful here. I wish you the best in using this strategy to fight AD, whether in yourself or a loved one.
And thanks to Paula and Anne as well, for the nice comments.
Makes great sense. I will start changing the way I eat. Unfortunately the person in our family who needs to heed this advice is incredibly stubborn and will probably not change a thing.
This is very dear to my heart and one of the many reasons I have completely gone to LCHF, and my entire family. I have shared so others can read this too and see the research above. Many thanks.
Thank you, Amy! This is the most useful written information I have seen so far on dementia. I’ve been a caregiver (who studies nutrition) for years, currently with a client who has “frontal lobe dementia”. I will copy your article for an appointment with her neurologist this week.
My client, at 57yrs, had a brilliant managerial nursing career, is very physically active, still plays tennis and works out at the gym, but speaks very repetitively and does not have ‘boundaries’ with other people. She is almost like a combo of autism, bipolar, and idiot savant. Her brain scans show a large black spot in the frontal lobe.
I’m giving her bone broth every day I am with her, and I’d like to add lacto-fermented foods. She does have gas and digestive disturbance. When you mentioned oxidative stress in the brain, I wonder if larger amounts of Vitamin E might help to protect the cells?
Your article has given hope. Thank you!
Hi LHay — I’m not sure if vitamin E would help. Maybe a little, but really, probably any good antioxidant would help. Alpha-lipoic acid looks promising, but the real key is a drastic dietary shift to put the brakes on such rampant oxidative stress in the first place. 57 is way too young for cognitive issues! My sincere good wishes on being able to help your client. -Amy
Thank you, Amy. I am currently battling this. I am 45, discovered i was having high blood sugar levels over 500 and immediately changed my diet. I keep it under 120 with eating mostly raw greens, celery,asparagus, avocados, pasture raised eggs,cultured butter and pecans.NO carbs, no fruit, no meat. I was having horrible memory problems during the time i was trying to figure out what i could eat. Methlyfolate Plus by Biotics helped and taking food enzymes, especially Lipase helped too. I still forget things that I should remember, but it’s much better now. I’m still learning and discovering how to gain my energy and memory back to optimal levels, and I appreciate your article! I will share with my alternative dr.!
Hi Tracy,
Just curious — why no meat? Meat has the full complement of amino acids — very important for whole-body health, including the brain. (Glad to hear you’re eating eggs, though! When you eat a very low carb diet, animal foods are extremely important!) Please let me know if I can be of any help.
Great article! Such good presentation of plethora of info, I have hope I can get others to actually read it. Having taken care of AD patients it’s my experience that most of them practically live on sugar. I don’t know if they’ve always eaten so poorly, or if it’s a result of low cognitive function by the time I see them, but I’m regularly amazed at the amount of candy, and the absolute lack of any other nutrients, consumed. I always wish I could do a survey of their earlier years to find out prior eating habits. Based on this info, I’m betting I know.
Would it be possible that an AD patient has sugar cravings because of the disease?
Hi Diana,
I don’t know that we can say AD would *cause* cravings for sugar, but certainly many AD patients are “sugar junkies” — as described by themselves and their families. So the two might go hand-in-hand, but in my opinion, it seems to be glucose & insulin dysregulation that’s causing AD, rather than the other way around.
Wow, what an amazing article! Thank you, Amy. My mother recently passed from AD and I have been trying to gain more understanding of the disease process and causes.
I, myself, have been a sugar addict for many years and have known I should get it under control for obvious, reasons. However, I have found it difficult due to the cravings. Your article just gave me the incentive I need. No more fooling around…I am making changes!
Thank you again for sharing this knowledge.
Glad you found it useful, Bobbi! I’m not sure what your current diet is like, but if you’re really a sugar addict, you might consider looking into some of the good lower-carb plans out there — Wheat Belly, Protein Power, etc. You can reprogram your body to run on a primarily fat-based metabolism, rather than carbohydrates, and you’ll get off the blood sugar rollercoaster, and avoid the need for constant snacks throughout the day to “keep your blood sugar up.” (Hate that nonsense!) Diane SanFilippo’s 21-day Sugar Detox is a great way to start, too. Lower-carb is usually recommended for weight loss, but even if body weight is not an issue for you, it’s still a good way to go for overall health and, of course, mitigating/preventing the effects of carbohydrate over-consumption.
Excellent article. I wish Mrs. Obama would read it.
My wife and I originally went low carb, a number of years ago, to lose some pounds that had crept on (20) while eating a very low fat, Dr. Ornish style diet. After studying available information about the low carb diet, we no longer consider processed carbs, starches or sugar to be food. We just wish we had known before while we were raising our children. Only one has adopted the lifestyle and she has done very well with it.
I found your blog through a link on the locarbdietition. It was a link to your blog article about Metabolic Theory of Cancer. Excellent, fascinating content that should also be read by everyone.
One night, my wife sat up in bed and said “someday, and it won’t be in our lifetime, everyone will eat this way because everyone else will……….be dead.”
Hi.
What a great article! I’ve been searching for this kind of information. My mom has AD and what worries me is that the degeneration is not only mental but also physical. Two of my uncles also had AD, but remained physically strong to the end. She is losing a lot of weight and I’m wondering if this can be linked to the underlying diabetes? Any response would be appreciated.
Irma
Why is it, that the cost of eating healthy is 10 times higher than the processed, refined, chemically enhanced foods?
Why are the organic fruits and vegies twice as expensive.
I thought chemicals, antibiotics, pesticides etc.. all cost $$$ ??
Whereas dirt, compost, and manure are free?
We wonder why we have diseases like ad, autism, autoimmune, cancer?
Its only going to get worse, with so many people in poverty, who can only afford to eat processed, refined, chemically addicting foods we don’t stand a chance. And for those of us who grew up in poverty the damage is already done.
I don’t have ad yet, but at 48 yrs I have had cervical cancer, degenerative disc and joint disease, now an autoimmune explosion including hashimotos, sjogrens, raynauds, and now lupus with seid/cfs/me I no longer function.
It’s pretty bad when you can’t even stand yourself. (inside joke about the body attacking itself)
Im not diabetic, but I am overweight. Im not lazy or a pig. I do not live to eat, I eat to live. But when your metabolism doesn’t function if you eat you will gain weight regardless.
Todays medical industry is a sham.
We Americans should be ashamed of ourselves for letting that almighty dollar cost us our freedom !!
Freedom from diseased minds and bodies
What’s a poor girl to do?
Sincerely,
Denise Porter
Hi Amy, Excellent article.
” … there is something interfering with the proper binding of what little insulin is present. ” … I suspect it is Trans Fats in the cell wall (fat membrane). Average US consumption of Trans Fats is 4.6 lbs (2.2Kg) p.a. A Canadian study found human breast milk contained 6% trans fats.
Trans Fats: German patent 141,029 in 1902 by Wilhelm Normann, found in many processed foods.
I completely reversed my Diabetes type 2 by a total ban of Tran fats from my diet. My hypothesis is that Trans Fats are ALSO the root cause of Alzheimers disease.
I published a short eBook (8 pages) on how I completely reversed my Diabetes Type 2 in 7 months and sent a copy to Michelle Obama in 2012. Barack Obama has now banned Trans Fats for all 350 million US citizens from 2018, The EU may have to follow – 450 million ….. smiles allowed!
Difficult to ban Trans fats from your diet but a rule of thumb is avoid all packaged / processed foods including chips in packets or from fast food outlets.
A very interesting and informative article.
I’m curious why there is no mention of Type 1 diabetes and its relation/connection to AD. My daughter (age 40) and granddaughter (age 15) are both Type 1 diabetics and have been taking insulin (4x daily) for over 8 years.
Would appreciate advice in this regard.
Thanks
A type 1 diabetic will always need to take insulin as it is necessary to life, but they do NOT need to become insulin resistant and should be on a low carb, high fat diet.
What a great article. This kind of information is that I always look for. In June of 2015, it was discovered that I had type 2 diabetes. By the end of the month, I was given a prescription for Metformin. I stated the ADA diet and followed it completely for several weeks but was unable to get my blood sugar below 140. With no results to how for my hard work, I panicked and called my doctor. His response? Deal with it. I began to feel that something wasn’t right and do my own research. Then I found Rachel’s blog http://myhealthlives.com/i-finally-reversed-my-diabetes/ . I read it from cover to cover and I started the diet and by the next morning, my blood sugar was 100. Since then, I have a fasting reading between the mid 70s and 80s. My doctor was so surprised at the results that, the next week, he took me off the Metformin. I lost 30 pounds in the first month and lost more than 6 inches off my waist and I’m able to work out twice a day while still having lots of energy. The truth is we can get off the drugs and help myself by trying natural methods
I think I have a version of diabetes that’s not type 1 or 2…If it’s not 3, there may be a diabetes 4! It’s hell thats all I know.
A very interesting and informative. Have shared and posted it far and wide amongst friends, nutritionist and herbalists.
I cannot pretend to understand everything in this article, but there were some parts that stood out, especially as regards supplementation and low-carb high-fat diet. I have recently embarked upon the keto way of eating and have added most of the supplements mentioned. Hopefully, in about six months, my brain fog will have lifted sufficiently that I will be able to re-read this article and get more out of it. Thank you for publishing this information. I will be coming back from time to time to absorb as much of it as I can!
Get Dale Bredesen end of Alzheimer’s on Amazon, lays it out very clearly, good luck.
I have been caring for my mother in law who has dementia for the past 10 years. Over the years I have also chatted with other carers who are looking after people with dementia. As long term carers we have noticed broad trends. Many dementia patients have certain things in common: Before getting dementia they were all taking statins and gout medication. They all had regular flu shots before getting dementia. They all consumed a lot of diet drinks; artificial sweeteners, salt substitutes and were on diets that avoided fats before getting dementia: Most were diagnosed with type 2 diabetes before getting dementia. Most had one or more general anaesthetics due to surgery before getting dementia. Most had hormone replacement therapy before developing dementia. After getting dementia they were/are constantly craving sugar. Left to themselves they will drink a litre of coke in a couple of hours or eat a jar of jam within a day or an entire packet of chocolate biscuits in an hour. The sugar in jam and chocolate also makes their dementia symptoms worse and makes them moody or aggressive. Fats like coconut oil and herbs like Valerian help reduce the mood swings. Activities like colouring in really help with the mood swings.
Exactly as laid out in Dale Bredesen’s book “end of Alzheimer’s” use of MCT oil to feed the brains energy requirements
The best synopsis of the subject I have ever seen. If there was no counter intention to creating and sustaining health, this along with Joe Craft’s work on diabetes and insulin resistance, would be required reading. BTW, the woman who made this all possible was the 1977 winner of the Nobel Prize in Medicine, Rosalind Yallow, who has had her work on testing insulin ignored.