





 🖨️ Print post
🖨️ Print post
At least one in three people will develop type 2 diabetes in their lifetime.1 I am in my sixties and have type 2 diabetes, which is particularly common in older adults. Over one-fourth (25.9 percent) of Americans age sixty-five and older have some form of diabetes, and over half (51 percent) are prediabetic.2 If you’re walking down the street and see someone over sixty-five, it’s highly likely that that person is prediabetic or diabetic.
As a psychiatric physician, I am not a diabetes expert, but I have learned a lot about it in the twelve years since I became ill, and I continue to learn. When new information comes along that seems worthwhile, I share the it, even if it contradicts prior information. Most importantly, I am a firm believer in the importance of eating a Wise Traditions diet if you have type 2 diabetes. Were it not for the information that I obtained through the Weston A. Price Foundation, I would have been disabled, at the very least.
HOW DIABETES DEVELOPS
To understand how type 2 diabetes develops, there are little islets of beta cells clustered in the pancreas, and everyone is born with a certain number. Beta cells produce and secrete insulin. Science is still learning about the life cycle of a beta cell, but we think that when there is a metabolic stressor, the beta cells start producing more insulin. We haven’t even identified all the metabolic challenges that elicit this response, but we do know that once the beta cells are taxed, consuming a lot of carbohydrates can be hard on them.
When beta cells start putting out volumes of insulin, a funny thing happens. It’s as though the beta cells don’t want to have the stress of this bombardment, so they abdicate their job and turn into some other cell, almost as though they were saying, “This executive job is really tough so I think I’ll go to the mail room instead.” It’s unclear whether beta cells can recover in type 2 diabetes in humans (animal studies suggest they can under certain conditions), but what is known is that by the time you are prediabetic or stage one diabetic, you may have lost about half of your beta cells. That is one reason why a person should pay attention to prediabetes rather than considering it a benign state. A lot of doctors will say, “Let’s just watch it,” but do you really want to watch it until it turns into full-scale diabetes? I wouldn’t accept that for an answer.
Physicans use the hemoglobin A1c blood test to estimate average blood sugar in the preceding two to three month period and determine if the average blood sugar levels are too high. However, the hemoglobin A1c test is not always reliable because factors such as how fast your blood cells turn over can affect the results. To assess diabetes, it is best to look at other factors as well.
In fact, there are a number of clues that indicate someone may have diabetes. These include the presence of metabolic syndrome and high blood pressure. You typically see metabolic syndrome in the apple-shaped person. If you’re an apple, you’ve got fat underneath that beautiful layer of muscle surrounding your organs, sort of holding the organs hostage inside. (If you’re a pear, you tend to gain weight in the hip and thigh area, a healthier place to gain.)
A skin condition called acanthosis nigricans (defined as velvety darkening of the skin, usually found in body folds) can also signal high insulin levels. It doesn’t mean you definitely have diabetes or prediabetes, but it’s something to note. Other possible diabetic clues include problems with foot sensation, problems with eyesight, gum disease and tooth loss. Many dentists are starting to diagnose diabetes in their patients. Sleep apnea, too, can promote or worsen diabetes, so snoring is not an innocent thing. Sleep deprivation stimulates evening cortisol, promoting high insulin levels and insulin resistance,3 so people who do not sleep well definitely should be checked. It also can be important to note a history of being a large baby, having a large baby or having gestational diabetes. Polycystic ovary syndrome (PCOS) can be indicative of insulin resistance. Fortunately, women with PCOS sometimes can get their fertility back if they eat a diet high in good fats and low in carbs.
A PERSONAL EXPERIMENT
I have been on a low-carb diet for about ten years now. I recently did some personal experiments with sugar and starch. I want to share them with you, prefaced with the caveat that my metabolism may not be like yours because diabetics respond differently than people who are not diabetic.
A Dexcom G5 system provides continuous glucose monitoring. One tiny part is a transmitter; it has a hair-like sensor that painlessly goes underneath the skin. It tells its story to your watch or phone or to its own device. It can lose its accuracy over a day or so, however, which means that you have to calibrate it twice a day with a blood drop glucometer. It is more often used by patients with type 1 diabetes. I bought one to be able to do this experiment. (As a side comment, glucometers only measure glucose, so if you are worried about the effects of something like agave nectar, which can be up to 95 percent fructose, a glucometer will not be of any help.)
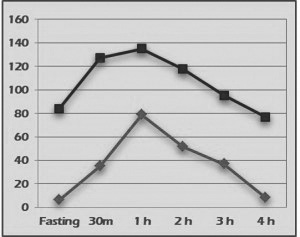
I made sure that I had eaten carbohydrates before I did these experiments, because I wanted to gear my body up and not produce false results. After years of not eating candy, the first part of my experiment was to eat two fun-size Snickers chocolate bars containing twenty-one grams of carbohydrates, eight grams of fat and one gram of dietary fiber. Post-Snickers, my Dexcom glucometer measure went up to a high of about one hundred and thirty-six. For a diabetic, that’s pretty good, but it was only twenty grams of carbohydrates. When health care providers administer a glucose tolerance test, they give you almost four times that amount of glucose (seventy-five grams). The ideal fasting blood glucose number is usually less than eighty-six. On an oral glucose tolerance test with seventy-five grams of glucose, the number should be no higher than one hundred and forty after a meal and, two hours after the meal, no higher than one hundred and twenty. After three hours, it should go back to the baseline.
Next, I tested the concept that starch is sugar by eating unsweetened, whole grain Cheerios. Following directions on the side of the box, I paired the Cheerios with fat-free milk. This meal had about 23.5 grams of carbohydrate.It was the first time in many years that I had consumed skim milk. Careful measurement showed that my Dexcom number rose to almost two hundred. This is like the crack cocaine of carbohydrates—even seventy-five grams of glucose during my glucose tolerance test did not push my sugars as high as the Cheerios-skim milk combination!
Livestock farmers in the early 1900s knew that skim milk and grain deliver the best economic returns in terms of fattening swine. Hogs relish the grain/skim milk combination and can’t get enough of it. Hogs that consume grain and skim milk are always hungry and will practically eat themselves inside out.
A farmer I know confirmed this. She feeds her meat pigs skim milk and grains, but she feeds her breeders healthy food.
For over a decade, I have been eating foods such as sausage and omelettes with cheese and heavy cream. These are very filling for me. I don’t need that many calories because I’m loaded up with good protein and fat. However, as soon as my blood sugar normalized after my Cheerios experiment, I was famished. I had not experienced that kind of hunger since I began eating a Wise Traditions diet. I was surprised. Even though I returned immediately to my “go-to’s” (sausage, eggs, butter), and avoided carbs after that, I had a hard time feeling satisfied with my food for about two days.
MONITORING GLUCOSE
If you have type 2 diabetes, it’s great to use a glucometer to estimate where you are metabolically and how your body responds to different foods. A glucometer can be your best friend. Glucometers themselves are inexpensive, but where they hit your pocketbook is with the strips. However, if you buy a month’s supply of strips, you can learn a lot, and what you learn can help you with your eating choices.
If you want to experiment, use a glucometer to measure your fasting blood sugar level when you wake up, just before a meal. Measure your blood sugar one hour later, then two hours later to see how your blood sugar responds to your meal. For guidance, see below (U.S. units):
Marker …………………………………………………………..Ideal
Fasting blood glucose (mg/dL) ………………………..<86
OGGT/post-meal (mg/dL after 1 hour) ………….<140
OGGT/post-meal (mg/dL after 2 hours) ………..<120
OGGT/post-meal (mg/dL after 3 hours)
baseline Hemoglobin A1c (%) …………………………..<5.3
It is also a good idea to notice how you feel when blood sugar returns to normal after meals. Do you feel awful or do you feel good? Do you feel satisfied with your meal or are you still hungry? Do you have a few hours between meals where you are not thinking about eating?
It is interesting to compare oral glucose tolerance test curves for someone with normal blood sugar and someone with type 2 diabetes. Looking just at blood glucose itself, in the type 2 diabetes test the number goes straight up—just like my two hundred number in the Cheerios experiment—but in a normal person, the number should go up to a maximum of one hundred and forty, but preferably lower. We are all a little different, and a seventeen-year-old with a healthy metabolism is likely to have different numbers than an elderly person.
I consume a very low-carbohydrate, high-fat ketogenic diet. In someone who makes enough insulin, a ketogenic diet stimulates “ketosis” (where the body burns fat for energy instead of carbohydrates) and not “ketoacidosis” (a dangerous condition in people who can’t make insulin, as in type 1 diabetes). It is comfortable for me to have blood sugar in the low 60s. My hunger is mild and cravings are rare, so my Cheerios experience came as a big surprise.
LOOKING BEYOND GLUCOSE
A meal with a steak and hollandaise sauce will have a much lower, more stable blood sugar curve than a whole wheat sandwich with an apple. It’s good policy to avoid foods that spike blood sugar this way. However, depending upon your situation you can get your diet “right” and still experience health problems and not lose weight. Nonetheless, with controlled blood sugar comes many other benefits, including more energy, clear thinking, better concentration and sleep. But when best efforts don’t yield benefits it makes sense to investigate further.
For example, a patient who had been on a low-carbohydrate diet for close to two years still had high morning glucose readings even though his daytime blood sugar was fairly low. They probably averaged in the nineties during the day, but as soon as he went to sleep, the numbers went up to one hundred and fifty and then dropped slightly to one hundred and forty. In this patient’s case, there was a problem with the liver, not the diet. The liver had been storing up glycogen, a type of carbohydrate from glucose, for a long time, and when growth hormone was produced overnight the glycogen (a liver “sugar”) spilled out as glucose into the blood.
Dr. Jason Fung is a Toronto-based kidney specialist, proponent of the Intensive Dietary Management approach to addressing diabetes and author of The Obesity Code: Unlocking the Secrets of Weight Loss and co-author of The Complete Guide to Fasting. Fung explains how the liver overfills with carbohydrate (glycogen). He uses techniques like eating within a certain time schedule and intermittent fasting to help rid the liver of glycogen overload.
Most people can fast 14 hours daily. If you want to do this it helps to take your body’s biological clock into account. Establish an eating pattern to fit into your job and routine. For example, you might have a ten-hour window of eating between, say, 7 am and 5 pm. Fasting between 5 pm and 7 am the following day gives your digestive system fourteen hours to rest. If your doctor agrees, you could also try periodic twenty-four-hour fasts where you might drink some bone broth with butter as your meal. For people with livers full of glycogen, intermittent fasting helps unburden the liver of glycogen stores so it can perform its normal functions.
INSULIN PATTERNS
During the last couple of years, I have become very interested in the work of Dr. Joseph Kraft, author of Diabetes Epidemic and You. Kraft’s viewpoint is that you may be able to monitor glucose with your glucometer, and that’s great, but it doesn’t tell you what insulin is doing. Insulin is the hidden black box problem, and until we can see blood glucose levels and insulin levels together, we can’t really know what’s happening.
I had a patient whose fasting glucose was consistently in the high sixties and seldom rose above one hundred and ten after meals, no matter what she ate. It turned out the reason glucose looked so good was that her insulin levels were sky-high. High insulin levels kept her blood sugar normal. If you only saw her glucometer, you would think her blood sugar levels were super, but her insulin test told a different story. That is why it’s important to look at insulin and glucose together.
Through his research, Kraft found that a combined glucose and insulin tolerance test could identify many more prediabetics than a simple oral glucose tolerance test.4 He identified six distinct glucose-insulin patterns: normal, delayed insulin peak, three patterns of insulin resistance, and insulinopenia (inadequate secretion of insulin).
In the normal pattern (pattern 1), insulin peaks during the first thirty to sixty minutes after you eat your meal at the same time that glucose rises to somewhere between one hundred and one hundred and twenty, and then both return to baseline together.
With a delayed insulin peak (pattern 2), glucose goes up right away. After a slight delay insulin increases to manage the glucose. Accompanying this graph, Kraft provides information that allows you to tell whether you have borderline or definite insulin resistance.4
Patterns 3A, 3B and 4 are all diagnostic for insulin resistance. In pattern 3A, as glucose rises the pancreas produces insulin too slowly. Pattern 3B shows even more problems with the output of insulin, capturing a high-sugar, low-insulin pattern where the beta cells are getting tired. Pattern 4 is also consistent with insulin resistance. Again, unless you check insulin before performing the glucose tolerance test and then every hour afterward, you won’t know this is happening.
Type 2 diabetes can become type 1 when the beta cells all but disappear, and this is the situation in pattern 5. Type 1 diabetics cannot live without insulin and at that point, there’s no getting around the fact that even if they adopt a low-carbohydrate, high-fat diet, they will need insulin in part because protein can be converted to carbohydrates via gluconeogenesis.
CARBOHYDRATES AND MOOD
Let me give you a little peek into my world as a psychiatrist. I have people who come in and think they’re bipolar because they have mood swings all day long. According to the definition of bipolar disorders in the latest edition of The Diagnostic and Statistical Manual of Mental Disorders (DSM-V), however, those moods should last at least a few days and be consistent.
What else might be going on here? What these people are doing is challenging themselves with more carbohydrates than their bodies can handle. It makes them irritable and gives them hungry-angry mood swings. When they eat the type of nutrient-empty carbohydrates that turn to sugar fast, like pancakes with no butter and lots of syrup, it’s really hard on the body as it causes blood sugar (glucose) to spike. Refined carbohydrate-rich meals favor high insulin production.5 Insulin grabs excess sugar and stores it as fat. That’s okay if they can access the fuel between meals, but the presence of insulin locks this fuel away inside fat cells. As blood sugar drops they get hungry-and-angry (“hangry”). It’s natural to eat more carbohydrates to feel better quickly, but it makes the cycle start over again.
I ate a diet high in refined carbohydrates, most of my life. I nearly fainted from hunger sometimes and couldn’t make it to lunchtime without snacks. I tried hard to stay slim, but carbohydrate cravings were out of control. I had to eat every few hours. Frequent hunger and low blood sugar is one reason people who follow high-carbohydrate diets are advised to eat frequent small meals.
Imagine if a bushman of the Kalahari desert whose job it is to hunt gazelles has to eat every two hours during an eight hour hunt. As persistence daytime hunters, primitive humans could walk, jog and run eight hours or longer to capture one buck. If they had to eat every two to three hours, they could not hunt large game and their families would go hungry. Humans were not meant to eat six times a day, as Americans do with their high carbohydrate, lowfat foodways. It is natural for human beings to be free to do other things and not be preoccupied with frequent meals.
CRITERIA FOR THE KRAFT PREDIABETES PROFILE
Upper line represents glucose levels; lower line represents insulin levels
 PATTERN 1: NORMAL
PATTERN 1: NORMAL
Normal fasting insulin 0-10 units
Peak insulin at ½-1 hour
2nd hour insulin <50
3rd hour insulin < 2nd hour
2nd hour + 3rd hour totals < 60
Subsequent values at fasting range (0-10)
PATTERN 2: DELAYED INSULIN PEAK
Normal fasting insulin 0-10 units
Peak insulin at ½-1 hour
2nd hour + 3rd hour totals > 60 and <100 = Borderline insulin resistance
2nd hour + 3rd hour totals > 100 = definite insulin resistance
PATTERN 3A: INSULIN RESISTANCE
Normal fasting insulin 0-10 units
Peak insulin at 2nd hour
Considered diagnostic for insulin resistance
Glucose tolerance may be within normal limits or impaired
PATTERN 3B: INSULIN RESISTANCE
Normal fasting insulin 0-10 units
Peak insulin at 3rd hour
Considered diagnostic for insulin resistance
Glucose tolerance usually at diabetic levels
PATTERN 4: INSULIN RESISTANCE
Fasting insulin >10
Diagnostic for insulin resistance
Glucose tolerance usually at diabetic levels
PATTERN 5: INSULINOPENIC
When glucose levels are elevated, this is considered a Type I DM pattern
All tested values for insulin <30
Insulin insufficiency probably due to damaged or exhausted islet cells
Glucose tolerance usually at diabetic levels
May signal the need for exogenous insulin
When seen with normal glucose values, may indicate a low-carbohydrate diet
Source: Dr. Joseph Kraft, Diabetes Epidemic and You
LOW-CARB, HIGH-FAT DIETS
Let’s start with definitions:
• Moderate-carb diet (MCD): 130-225g carbs daily and between 26-45% of calories (in 1979 before obesity struck, Americans ate 43% of caleries as carbs).
• Low-carb diet (LCD): 50-130g carbs daily and between 10-26% of calories.
• Low-carb ketogenic diet (LCKD): less than 50g carbs and 10% calories daily.
Since dietary protein requirements remain constant, additional protein does not fill in for the loss of carbohydrate calories; additional fat does. As it turns out, fat does not promote insulin as carbohydrates and, to a less extent, proteins do.
Some experts say that you can cure noninsulin-dependent type 2 diabetes with a nutrient-dense, low-carb and high-fat diet. I don’t know whether this is the case for humans, but there is recent news about promoting insulin producing new beta cells in mice via fasting. Still, whether being on a low-carb, high-fat diet can revive human beta cells or not, I believe it is the best way to put type 2 diabetes into remission.6 Once blood sugar normalizes you can challenge yourself or experiment with different foods and use your glucometer to measure your response. By the way, it’s important to know that a low-carb, high-fat meal does not exclude protein. It includes moderate protein intake in the form of foods like meat, fish, shellfish, eggs and poultry, with all the fats nature gave them.
Typically, weight normalizes with a low-carb, high-fat diet, as do hemoglobin A1c and glucose. HDL-cholesterol (“good cholesterol”) increases reliably and triglycerides decrease. Triglycerides are driven by alcohol, carbohydrates and fat loss. By and large, if your triglyceride number is seventy or less, your good LDL-cholesterol—the large, fluffy, friendly kind—rises to a safe level. High triglycerides, on the other hand, raise your risk of having the bad kind of LDL which is small and dense, the kind driven by refined carbohydrates. One exception is people who are losing weight on a low-carbohydrate diet. They may temporarily have high triglycerides and the good kind of LDLs as fat stores are consumed by the body for energy.
One person who is a first-hand expert on the effectiveness of this type of diet is Dr. Richard K. Bernstein, who was an engineer right around the time the glucometer was invented. Bernstein had type 1 diabetes and worried about his poor health. He started eating certain foods and tested himself with a glucometer, taking copious notes and measurements with everything he ate. In the end, he believed he had figured out what to do. He wrote a book based on his successful personal experiments but couldn’t find a publisher because he had no medical degree. So he went to medical school and after he earned his medical degree, his highly regarded book—Diabetes Solution—was published.
Type 2 diabetics can experiment with a range of carbohydrate intakes, but it is essential to ensure that all carbohydrates are properly prepared prior to eating them. This means soaking, souring (fermenting) or sprouting. All of these techniques decrease carbohydrates. Have you ever sprouted a bean, watched it split and seen the little ears on either side turn green? This is a sign that you are turning on enzymes that are using up some of the carbohydrates, in addition to getting rid of antinutrients. While you may not see green in a sprouted nut or grain, carbohydrates are still being consumed to some degree.
Some studies show that bread that is soured or made of sprouted grains does not provoke blood sugar spikes to the same extent that white bread does.7,8 However, some type 2 diabetics experience spikes even from sprouted grain bread. Believe it or not, whole wheat bread is the very worst culprit and causes worse blood sugar spikes than white bread.
There are special considerations for persons who are prediabetic or diabetic but have no gallbladder. Nonetheless, a lot of my patients who don’t have a gallbladder do fine with butter. Certain fats are easier than others. Most people are fine with coconut oil because it doesn’t need bile for digestion. There are supplements you can take to help your digestion and things you can do to help your liver to compensate, such as always eating at fixed times. Ox bile extract can help with absorption of dietary fats.
Of course, a low-carb, high-fat diet can be a tough sell in a world where Big Sugar spends millions to persuade countries around the globe that sugar is safe and even healthy.9 In South Africa, Professor Tim Noakes (author of The Real Meal Revolution and Raising Superheroes) was called before the Health Professions Council for daring to advocate the removal of sugar from children’s diets while emphasizing the importance of fat for brain development.10 Likewise, Australian physican Gary Fettke was silenced by the Australian Health Practitioners Regulatory Authority for his promotion of lowcarb, high-fat diets for some patients and his willingness to condemn sugar and junk food.11
ELEMENTS OF TREATMENT
When adopting a low-carb, high-fat diet, it is vital that nutrient density be a top priority. People with diabetes especially need trace minerals, bone broth and high nutrient-dense foods like liver. I hated liver growing up, and was anemic by age 12. My personal “gateway drug” to loving veal liver was chicken liver pȃté. Another good goal is to have properly prepared bone broth daily—with unrefined salt. No one should eat a low-sodium diet, as was recently confirmed in The Lancet.12 It is also important to avoid industrial vegetable oils. Soy oil, for example, is found to promote metabolic syndrome and diabetes in mice.13
An initial dietary treatment strategy for type 2 diabetes is to decrease refined fermentable carbohydrates to no more than fifty grams a day until glucose is stable. Fermentable carbohydrates are short-chain sugars that are easily fermented in the digestive system, and refined carbohydrates include foods such as bread, dry breakfast cereals and pasta. Your glucose monitor can tell you whether you are headed in the right direction. Be sure to reduce your carbohydrate levels gradually. You do not want to go into withdrawal and get headaches, dizziness and mental fog, which is sometimes called the “low-carb flu.” Change one meal at a time. For example, you can start with a low-carbohydrate breakfast and after a week, tackle lunch and then dinner. Monitor yourself for behavior and mood changes. In addition to diet it is helpful to exercise, as it promotes insulin sensitivity.
Avoid hypoglycemia at all costs. Studies show that the more hypoglycemic episodes diabetics have, the more likely they are to develop dementia.14 I think that’s why doctors are happy to keep glucose levels as high as one hundred and forty in elderly patients. However, if glucose can be safely brought below that level, that’s great. People with diabetes should be careful with alcohol because it can make them hypoglycemic. I did an experiment with just four ounces of wine when I had high blood sugar and it dropped my blood sugar rapidly.
Seek medical advice before starting any diet. For people taking medication, medical monitoring is necessary. For example, a lowcarb diet can lower blood pressure.15 This is the case, even when eating enough salt. Ideally you want to get off all medications if possible, but it has to be a gradual, medically supervised process. All drugs have side effects, and some of them impair one’s quality of life. Efforts to reduce or eliminate the need for medications are worthwhile.
TAKE-HOME MESSAGE
If you suspect that you have a metabolic problem, ask your doctor for a four hour oral glucose tolerance test with insulin. Make sure insulin and glucose levels are drawn before the test and at every hour afterwards. To stabilize your glucose levels, gradually reduce the intake of refined carbohydrates (starches and sugars). Remember that none of this is an exact science. We don’t have all the answers, nor do we have the answer for every person. A glucometer can guide you as to what to eat. It’s as though we who practice medicine just woke up to the fact that diet matters. We have a lot to learn. Thankfully, more and more people are starting to take control of their health. It is important to be an advocate for yourself and teach your doctor. Many doctors are open to being taught. I’ve learned a lot from my patients, for which I am grateful.
SIDEBARS
TYPE 1 AND TYPE 2 DIABETES
Type 1 and type 2 diabetes are somewhat different in their causes and treatments, but both involve impairments related to insulin.
TYPE 1: Type 1 diabetes (also called insulin-dependent diabetes) is an autoimmune condition thought to be set off by environmental or viral triggers. The body attacks the insulin-producing beta cells in the pancreas, causing the pancreas to lose its ability to produce any insulin at all. Type 1 diabetics require insulin therapy but also benefit from attention to diet and exercise.
TYPE 2: Type 2 diabetes can be viewed as a problem of “energy overload,” in which we consistently supply calories “in excess of our body’s capacity to burn them.”16 Over time, people with type 2 diabetes begin experiencing abnormally high blood sugar levels due to some combination of inadequate insulin secretion and insulin resistance17 (defined as “a state in which a given concentration of insulin produces a less-than-expected biological effect”).18 According to Dr. Tom Cowan, foods high in refined-carbohydrates that also include trans fats represent a “double whammy” in terms of their propensity to engender insulin resistance over time. With care, individuals with type 2 diabetes can manage their diabetes solely with diet and exercise.
DIABETES AND AGING
Prediabetes and diabetes affect about 75 percent of all seniors. Although there are many signs and symptoms to
look for, diabetes is mostly silent in the early stages, and that’s why many people don’t get diagnosed—they don’t know they have it. If you’re in a room full of seniors, it’s unlikely that 75 percent will raise their hands to say they have diabetes.
Due to some of the biological aspects of aging, it can be challenging for seniors with type 2 diabetes to eat well.
Older people’s nutritional requirements are higher, yet their calorie requirements are lower. The elderly also are more sedentary, and many have problems with digestion. What this means is that the elderly may not be able to assimilate nutrients as well as they could when they were younger.
Many other aspects of the aging process can affect older individuals’ dietary habits and digestion. Consider
dental health, for example. Many seniors may have worn or missing teeth or gum disease, affecting their ability to eat certain foods. Unfortunately, seniors with dental problems often favor easy-to-chew soft white carbs such as breads and pastas or canned goods. These processed foods are the low-hanging fruit that they find easiest to access, whereas obtaining good-quality fresh foods can require more effort.
With the altered sense of taste that can accompany aging, foods also may not taste the way they used to. Sometimes the sense of smell goes as well, particularly where dementia is present. As a result, seniors may not get the full experience from a bite of food. Eating something that is digestible and supporting the digestive process can make all the difference in the world.
People often do not realize that heavy sugar consumption and high glucose levels stiffen the arteries and the skin and can contribute to decreased stomach elasticity. Atrophic gastritis (chronic inflammation of the stomach mucosa) also is very common in the elderly, affecting almost one-third of adults over sixty. Atrophic gastritis can result from gastroesophageal reflux, use of medications that damage the stomach lining or other stomach problems. It is also important to recognize that liver metabolism changes as we age, making it harder for seniors to metabolize prescription drugs. Health care providers should be prescribing lower doses and exhibiting more caution with medications
for the elderly.
When people have dementia, they may not be able to prepare food for themselves or do the things they need to
do to take care of themselves. Some researchers call dementia “type 3 diabetes” because the effects of insulin resistance on the brains of persons with dementia. Diabetes, in fact, is a risk factor for dementia.19 However, symptoms of dementia can also result from vitamin B12 deficiency. My motto is, “You’re not demented until you’re nourished and demented.” I’ve seen people go from being completely nonverbal to talking and doing their work within a matter of months, simply by restoring vitamin B12 levels. It is important that every senior with cognitive symptoms be checked for B12 deficiency. Medline considers normal B12 values to be in the range of two hundred to nine hundred picograms per milliliter (pg/mL), but I like to aim for five hundred and fifty or higher, and some experienced practitioners recommend nine hundred or higher. At one time, I hovered in the three hundred range and couldn’t remember where I had parked my car. I started consuming a Wise Traditions diet, including bone broth and gelatin, and now my numbers are over nine hundred without supplements.
Because most older Americans do not eat a traditional foods diet, it is not surprising that many have problems
with ambulation resulting from osteoarthritis, arthritis or weak bones or joints. Sometimes people lose their cartilage. In these cases, bone broth is an essential rebuilding tool and also can reduce joint inflammation.
At least 15 percent of adults over age sixty suffer from mental illness, and many times, it is not their first episode. The lifetime incidence of mental illness is around 47 percent. That’s huge. Depression is very common in the elderly, and I would argue that a lot of it is diet-driven. Older people who perceive themselves as having mild dementia may, in fact, be depressed rather than having something wrong with their overall brain capability. Depression can also be linked to pseudo-dementia with loss of self-confidence.
Nearly a third of the elderly who live independently live alone. Some of them do not function well, and many
also have limited incomes. Malnourishment is common. I’ve heard of things as bad as pouring ketchup in water to make tomato soup. The mainstream dietary advice dispensed to these individuals is frequently counterproductive. For example, people are told not to eat liver because it has toxins and “is bad for you.” People with diabetes or prediabetes may be carbohydrate-sensitive, but they are not sensitive to good fats such as butter and lard, unless they’ve lost their gallbladder or have severe gallbladder disease. Unfortunately, many elderly people are educated by their doctors to fear fats, when good fats with their proteins, and fat-soluble vitamins are what they desperately need.
DIABETES: A DISEASE OF EXCESS OR DEFICIENCY?
While most of the medical community treats type II diabetes as something to be prevented through exercise and
healthy food, the rapid growth rate of the disease in developing countries calls for a more thorough approach. Ankita Rao reports that while visiting a rural hospital in Chhattisgarh, one of the poorest and hungriest states in India, she noted that the patients waiting in the corridors were thin and bony, with dangerously low blood counts and anemia. Yet the patients received treatment for diabetes and heart disease.
The public perception of type II diabetes is that it’s a disease of excess—the result of too much sugar in our diets
and a sedentary lifestyle. But this may be only part of the picture. Diabetes can burden people without enough food and nutrients, just as it does those who eat too much. In India, where people’s average weight and body mass index (BMI) is far lower than in the US, sixty-two million adults have diabetes, the largest diabetic population in the world. Rao observed pregnant women stand on weighing scales as the doctors went on village visits—many were just seventy-five pounds while seven months pregnant. Even so, experts have been attributing the uptick in diabetes to the sudden economic growth in the country—and the lifestyle and diet changes that followed. More junk food on the shelves, more access to carbohydrates and sugar, they thought, might be the culprit. But that couldn’t account for the largely poor population in rural areas.
Dr. Yajnik, a researcher and physician at Pune’s KEM Hospital Research Center, has been focused on this mystery for decades. He and his team conducted a longitudinal study in villages outside of Pune, where families still rely on farming as their main livelihood. His team tracked pregnant mothers and how their nutrition affected their children—mothers who would spend their days plowing the land or weeding until just days before their delivery. He found that the lack of one particular vitamin—B12—led to babies growing up with more visceral fat, despite their low weight in both their childhood and adult life. This then correlated to insulin resistance, the body’s inability to break down sugar properly, and a precursor to diabetes.
SOURCE: motherboard.vice.com/en_us/article/how-a-bmi-fallacy-convinced-the-world-that-diabetes-is-a-disease-of-excess
REFERENCES
1. American Diabetes Association. Infographic: a snapshot of diabetes in America. http://www.diabetes.org/diabetesbasics/statistics/cdc-infographic.html.
2. American Diabetes Association. Statistics about diabetes. http://www.diabetes.org/diabetes-basics/statistics/.
3. Fung J. Sleep deprivation and obesity-hormonal obesity. Intensive Dietary Management, Dec. 28, 2014.
4. Meridian Valley Lab. Kraft Prediabetes Profile: patterns overview. http://meridianvalleylab.com/Kraft-prediabetes-profile-patterns-overview.
5. Masterjohn C. Mastering Nutrition Episode 6: why “glycation” is a bad reason to restrict carbs. May 2, 2016. https://chrismasterjohnphd.com/2016/05/02/the-daily-lipid-podcast-episode-6-why/#transcript.
6. Feinman RD, Pogozelski WK, Astrup A, et al. Dietary carbohydrate restriction as the first approach in diabetes management: critical review and evidence base. Nutrition 2015;31(1):1–13.
7. Mofidi A, Ferraro ZM, Stewart KA et al. The acute impact of ingestion of sourdough and whole-grain breads on blood glucose, insulin, and incretins in overweight and obese men. J Nutr Metab 2012:184710.
8. Najjar AM, Parsons PM, Duncan AM et al. The acute impact of ingestion of breads of varying composition on blood glucose, insulin and incretins following first and second meals. Br J Nutr 2008;101(3):391-398.
9. Taubes G, Couzens CK. Big sugar’s sweet little lies. Mother Jones, Nov/Dec 2012.
10. News24Wire. “Remove sugar from your diet”: Tim Noakes. BusinessTech, Feb. 15, 2016.
11. No Fructose. Who has more to hide? http://www.nofructose.com/introduction/fettkeleaks/.
12. Mente A, O’Donnell M, Rangarajan S et al. Associations of urinary sodium excretion with cardiovascular events in individuals with and without hypertension: a pooled analysis of data from four studies. Lancet 2016;388(10043):465-475.
13. Deol P, Evans JR, Dhahbi J, Chellappa K, Han DS, Spindler S, Sladek FM. Soybean oil is more obesogenic and diabetogenic than coconut oil and fructose in mouse: potential role for the liver. PLoS ONE 2015;10(7):e0132672.
14. Yaffe K, Falvey CM, Hamilton N et al. Association between hypoglycemia and dementia in a biracial cohort of older adults with diabetes mellitus. JAMA Intern Med 2013;173(14):1300-1306.
15. Yancy WS Jr., Westman EC, McDuffie JR et al. A randomized trial of a low-carbohydrate diet vs orlistat plus a low-fat diet for weight loss. Arch Intern Med 2010;170(2):136-145.
16. Masterjohn C. Fat and diabetes: bad press, good paper, and the reemergence of our good friend glutathione [blog]. Weston A. Price Foundation, Aug. 30, 2011.
17. Khardori R. Type 2 diabetes mellitus. Medscape, Jan. 12, 2017.
18. Olatunbosun ST. Insulin resistance. Medscape, Jan. 30, 2015.
19. Mayo Clinic. Diabetes and Alzheimer’s linked. Mar. 23, 2016. http://www.mayoclinic.org/diseases-conditions/alzheimers-disease/in-depth/diabetes-and-alzheimers/ART-20046987.
DIABETES: A DISEASE OF EXCESS OR DEFICIENCY?
While most of the medical community treats type II diabetes as something to be prevented through exercise and
healthy food, the rapid growth rate of the disease in developing countries calls for a more thorough approach. Ankita Rao reports that while visiting a rural hospital in Chhattisgarh, one of the poorest and hungriest states in India, she noted that the patients waiting in the corridors were thin and bony, with dangerously low blood counts and anemia. Yet the patients received treatment for diabetes and heart disease.
The public perception of type II diabetes is that it’s a disease of excess—the result of too much sugar in our diets
and a sedentary lifestyle. But this may be only part of the picture. Diabetes can burden people without enough food and nutrients, just as it does those who eat too much. In India, where people’s average weight and body mass index (BMI) is far lower than in the US, sixty-two million adults have diabetes, the largest diabetic population in the world. Rao observed pregnant women stand on weighing scales as the doctors went on village visits—many were just seventy-five pounds while seven months pregnant. Even so, experts have been attributing the uptick in diabetes to the sudden economic growth in the country—and the lifestyle and diet changes that followed. More junk food on the shelves, more access to carbohydrates and sugar, they thought, might be the culprit. But that couldn’t account for the largely poor population in rural areas.
Dr. Yajnik, a researcher and physician at Pune’s KEM Hospital Research Center, has been focused on this mystery for decades. He and his team conducted a longitudinal study in villages outside of Pune, where families still rely on farming as their main livelihood. His team tracked pregnant mothers and how their nutrition affected their children—mothers who would spend their days plowing the land or weeding until just days before their delivery. He found that the lack of one particular vitamin—B12—led to babies growing up with more visceral fat, despite their low weight in both their childhood and adult life. This then correlated to insulin resistance, the body’s inability to break down sugar properly, and a precursor to diabetes.
SOURCE: motherboard.vice.com/en_us/article/how-a-bmi-fallacy-convinced-the-world-that-diabetes-is-a-disease-of-excess
This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly magazine of the Weston A. Price Foundation, Spring 2017.
🖨️ Print post
I have recently been diagnosed with type 2 diabetes. I am a 74 YO male from Australia, a member of WAPF who made ‘plenty of insulin’ and was accordingly obese.
I found the article very informative, but as this is going out to an international audience, it would be more informative if the numbers covered both the US and metric positions i.e. in Australia normal BGLs are 4.0 to 6.5mmol and diabetic levels are 5.0 to 8.0mmol
I have added Dr Jason Fung’s information and protocols into my diet and, for the moment, cut out ALL grains as I have found that even soaked grains sourdough breads shot up my BGLs, but Kombucha, beet kvass and raw milk and cream don’t cause any problems.
Watch out for kombucha as the fructose in the sugar does not get fermented. Fructose causes insulin resistance but fructose does not spike blood glucose.
Also from what I have learned blood sugar levels are only a symptom of diabetes yet it is treated as the cause of diabetes.
The actual cause of diabetes is insulin resistance which can be reversed and managed by eating a LCHF diet combined with intermittent fasting
See Dr Jason fung (Canadian nephrologist) on YouTube as well as the noakes trial on YouTube
Great article. Thanks for sharing this valuable information. I think a major contribution to the diabetes epidemic of our age is our lifestyle. There is so much talk about our diet. I am a male of merely 60kilos and must eat low carb to control my blood sugar. I rarely consume ANY grains and yet am by clinical definition, pre-diabetic. Insulin resistance must be the result of other contributing factors. Stress and circadian biology are massive. This is where our modern world of technology has us pegged. Our artificial light and screens have us living in an eternal summer. Where seasonally we eat carbs for endless months. We heat our homes for comfort and rarely expose ourselves to the elements. We are effectively disconnected from nature. Our genes still recognise the age old state of fasting and discomfort. Time for a shift in the paradigm.
Thank you very much for this informative text – very much appreciated! I’m a skinny, hard-working farmer in Ecuador, 50 years old, and thought I was eating a good nutrient-dense diet, but just at the point of being diagnosed with type 2 diabetes, and naturally somewhat shocked and anxious. It’s great to be able to access such high-quality info/opinion!
Thank you for sharing this information. I have been reading a lot about LCHF diets, diabetes epidemic, insulin resistance and I can tell this is a good resume. I have been following a LCHF diet since the last 15 months. It has been easy for me and I got used to. I am not taking meds for diabetes and my HA1b has drop from 6.7 to 5.4 %. 53 years old. Also I have lost 22 kg by the moment, now BMI= 23%. I feel better and more energetic. But my cholesterol numbers are not good enough. Here in Spain, LCHF diets are still not so popular than in other countries.
The use of plant foods as carbs was not addressed. Of course the non plant sources raise sugar levels, no secret there.
There are no studies, I have found , that don’t recommend more vegetables and fruits, even for diabetics.
Each group has its own agenda and will publish the parts that suppport that goal. I totally agree with the Wise Tradition life, but also feel there must be a strong use of plants as food.
Check out Mastering Diabetes
I’m a bit disappointed. I’m looking for gestational diabetes information on this site and this comes up.
ITS NOT THE SAME.
Its annoying that people assume it is.
Hormones are a factor with gestational diabetes.
It is why women who are healthy can become affected as well.
I know your comment is several years old, but i just wanted to point out that the article did not claim to be about GD. It came up in your search because you had “diabetes” in your search. For more specific search results, try placing quotation marks around your search terms like this “gestational diabetes”. This protocol would not be appropriate for GD because such severe restriction of carbohydrate as advocated here could harm the baby.
For years I controlled my type 2 diabetes with the highest recommended dosage of Metformin, but my blood sugar readings were always high, particularly in the morning. Eventually my doctor wanted to switch me to Glipizide, which has more side effects, but he agreed that eventually I’d have to switch to insulin, probably increasing over time, with increasing side effects. I decided that enduring a low-carb diet would be a better choice. But I soon discovered that there are ketogenic sweet foods of many kinds to satisfy my sweet tooth, there are several sources of near-pure protein, and I do love to eat cheese. So even though I don’t like cooking, I still keep in ketosis easily through my diet, without ever getting very hungry.
In recent years I have stopped measuring my blood sugar, because it was always in or near normal and my A1C readings are always in the normal range. Without any medication. And, yes, I had Stage 4 rectal cancer and recovered nicely from it about five years ago.
Two notes: 1. Doctors still often confuse ketosis with ketoacidosis. I think their training does not make this difference clear. How long will it take until the average doctor or specialist prescribes a ketogenic diet? 2. Walk through the aisles of most supermarkets and you’ll see that the majority of foods are mostly carbohydrates having differing taste and consistency. No wonder type 2 diabetes and obesity (and possibly Alzheimer’s Disease and others) are so high in modern society.
David Spector, Age 76
Portland, Maine
I have been diabetic Type 2 since 2003 I was on Metformin 850mg at night and 60 units Actraphane. my symptoms were cold feet weather it was warm or cold my feet were always cold especially at night, I also had severe neausa from taking metformin so this year my family doctor decided I should try alternative treatment as Metformin caused severe side effects; I agreed and decided to start the Diabetes protocol offered at Uine Health Centre. my symptoms have greatly improved with no signs of blurred vision which I always seem to use to have or the frequent thirst. No more numbness of my feet I’m active again which has helped me loose weight. Since starting the diabetes formula my A1C is back to normal range and my blood sugars have stated normal. I’m surprised a lot of people with Diabetes T2 haven’t heard of the formula. Visit uine healthcentre . c om