





Measles has been in the news a lot lately. It therefore seems timely to fulfill my now more than two-year-old promise to write a blog on the possibility and evidence that cod liver oil may have contributed to the historical decline in mortality from measles and other infectious diseases.
I made that promise in a blog post about the contribution of family planning to the historical decline in infectious disease mortality. I will reiterate the relevant background from that post in this one, but for the full treatment of these background issues I recommend reading that post itself.
Conventionally, public health historians attribute the decline in infectious disease incidence and mortality to interventions that helped stop the spread of microorganisms, such as sanitation, hygiene, identification of infected individuals so they could be treated and the risk of transmission could be minimized, as well as specific vaccinations and medical treatments.
In his 1976 The Modern Rise in Population, Thomas McKeown focused on the other half of the equation: changes that improved the resistance of humans to infectious diseases. In particular, his argument centered on improved “nutrition.” To McKeown, this meant not an improvement in food quality but an improvement in food quantity. That is, as farming methods improved, fewer people were food insecure and more people had access to adequate food, including access to all the macronutrients and micronutrients needed to support immunity.
In my previous post, I described and critiqued a 2010 argument that Ostry and Frank published in the journal Critical Public Health under the title “Was Thomas McKeown Right for all the Wrong Reasons?” They suggested that, although McKeown did not give enough credit to specific public health interventions, he was likely right that improved food availability drove the nineteenth century decline in adolescent and young adult tuberculosis mortality. They also argued, however, that declines in mortality from measles and other infectious diseases were part of a later trend that primarily affected infants and young children and did not begin until the 1890s. This trend, according to their argument, resulted from improved family planning. As families increasingly and purposefully restricted their sizes, mothers were better able to conserve vitamin A, iron, and other precious nutritional resources that they must supply to their unborn children and nursing infants in order to provide them with robust immunity to infectious diseases.
In that post, I agreed with Ostry and Frank that improved family planning likely mitigated the toll of infectious diseases but I argued that it couldn’t have in and of itself resulted in the massive increase in modern population, the phenomenon that McKeown had been trying to explain and after which he titled his book. McKeown himself had presented data showing that the proportion of children surviving increases as family size decreases; nevertheless, the improvement was not sufficient to allow people to have more surviving children simply by giving birth fewer times. In order to explain how the decline in infectious disease mortality resulted in a population boom, one has to explain how mortality could be reduced more than family size had decreased so that there would be a net increase in surviving offspring. I concluded by promising a future post in which I would explore the possibility that the rise in the popularity of cod liver oil and the consequent improvement in vitamin A status could explain part of the historical decline in infectious diseases.
While McKeown, and Ostry and Frank after him, were concerned with how the decline in infectious disease mortality contributed to the population boom, my argument above is interesting to me not so much because I want to explain the population boom, but because it implies that there is still more to be explained about how infectious disease mortality was virtually eradicated. Herein, I will argue that improved nutritional status of vitamin A, especially from cod liver oil, is an important piece of the puzzle.
Cod liver oil had been used from time immemorial by the fishing populations of Scotland, Sweden, and Norway. In 1771, the physician Percival added it to the British pharmacopeia after showing it was more effective than a placebo at treating rheumatism. By the 1820s, its use in medicine had become widespread in Germany, Holland, and the Netherlands. Physicians used it to treat rickets at least as far back as 1799, and in the nineteenth century they expanded its uses to the treatment of xerophthalmia, an infectious disease of the eye, and tuberculosis, then the leading cause of infectious disease mortality.
Resources for further reading on the history of cod liver oil include John Hughes Bennett’s 1848 Treatise on the Oleum Jecoris Aselli or Cod Liver Oil; RA Guy’s 1923 review in the American Journal of Diseases in Children, The History of Cod Liver Oil as a Remedy; and Mark Kurlansky’s 1998 Cod: A Biography of the Fish that Changed the World.
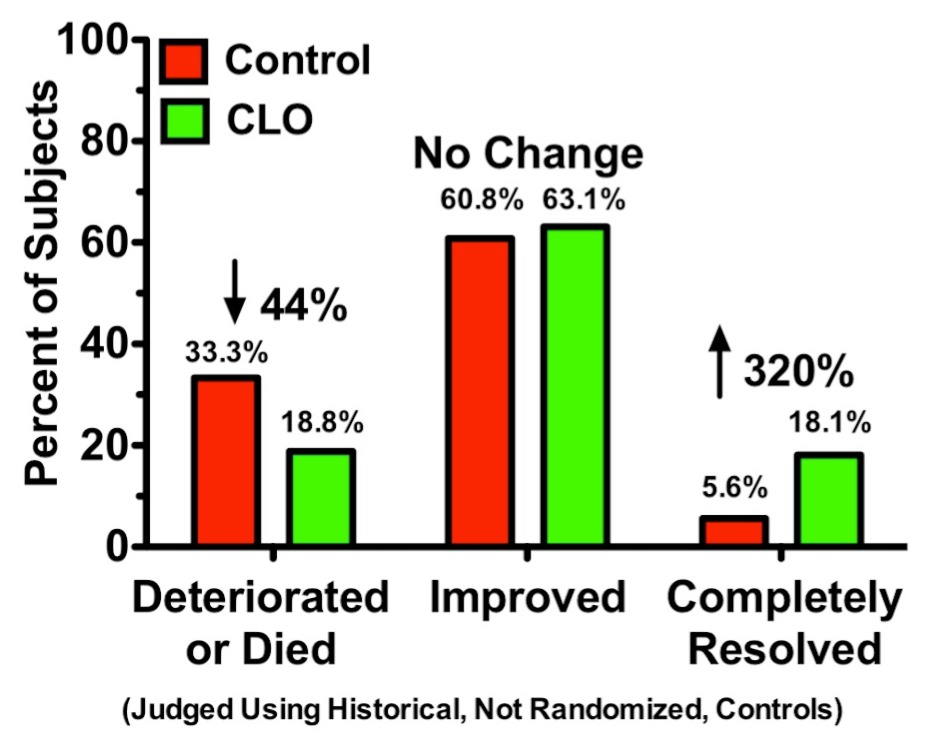
In 1848-9, London’s Royal Brompton Hospital published the results of their first five years using cod liver oil in the treatment of tuberculosis. Malcolm Green revisited these data in the British Medical Journal in 2011. I created a graph depicting these results, shown below. Compared to how patients fared before they began using cod liver oil (CLO), patients treated with CLO were over three times as likely to completely recover and their risk of deteriorating or dying was almost cut in half.
I do not have data on the rate at which cod liver oil was imported into Britain but the United States was importing about two million pounds of cod liver oil per year, and I am guessing the bulk of it was used to treat tuberculosis, following the positive experience demonstrated in Britain.
The nineteenth century also saw the use of cod liver oil expand to the prevention and treatment of rickets, a bone disease now known to result from a deficiency of vitamin D, and xerophthalmia, an infectious eye disease now known to result from a deficiency of vitamin A. In the early twentieth century, scientists discovered and characterized vitamins A and D. During this early burgeoning of nutritional science, the pioneers of this science promoted the use of fresh whole foods over refined and processed foods. They also promoted the use of colorful vegetables, organ meats, and animal fats related to reproduction, especially butter and egg yolks, as sources of fat-soluble vitamins. While I have no data to directly support this, I suspect that nutritional status of vitamins A and D and micronutrient status in general improved during this time.
We should keep in mind that micronutrient status was likely improving from one of its lowest points in human history: humans began the industrial refining of foods first and discovered the existence of the nutrients lost during those procedures only after they were suffering from widespread deficiencies. Prior to the industrial refining of foods, I am guessing that the greatest periods of nutritional deficiency were those involving famine and food insecurity as well as those involving the agricultural production of a single crop or small numbers of crops that displaced other important foods.
The two decades between 1920 and 1940, were the golden age of vitamin A status. Sir Edward Mellanby, credited with discovering vitamin D, performed experiments in animals with his colleague Harry Norman Green showing that vitamin A had singular power to protect against infections of the tongue, throat, eyes, lungs, and gastrointestinal tract.
These experiments popularized the concept that vitamin A was the “anti-infective” vitamin. Semba reviewed this era in his 1999 review, “Vitamin A as Anti-Infective Therapy, 1920-1940“. He later expanded his historical research into a book, which I have not yet been able to read, The Vitamin A Story: Lifting the Shadow of Death.
Cod liver oil or concentrates of its vitamins were shown in numerous clinical trials during that era to reduce the incidence and mortality of infectious diseases such as the common cold, bedside fever, and measles. One study, for example, found that a concentrate of vitamins A and D reduced measles mortality from 26 in a 300-person control group to 11 in the 300-person treatment group. Thus, vitamin therapy cut measles mortality by about 58 percent. A recent meta-analysis of modern literature on supplementation of vitamin A alone found that supplementation could cut measles incidence in half. If one were to simplistically combine these figures one would arrive at the conclusion that halving measles incidence and then cutting the proportion of cases that result in mortality by 58 percent could reduce total measles mortality by just shy of 80 percent.
One could argue that this would overestimate the prophylactic effect of widespread increases in vitamin A status: perhaps these clinical trials targeted populations likely to be deficient in vitamin A, whereas blanket recommendations to increase vitamin A status would do little for broad swaths of the population who are not deficient.
On the other hand, one could also argue that this underestimates the effect: if vitamin A is protective against both incidence and mortality, it should have the best chance of being effective when vitamin A status becomes optimal long before exposure to the virus so that vitamin A stores can truly be replete by the time one encounters high-risk exposure, and so that any of its long-term effects — especially its effects on tissue development, which take place over the timescale of months to years — can be actualized prior to high-risk exposure.
Indeed, I would argue that the historical data are, while not a basis for making a certain conclusion about cause-and-effect, at least consistent with the latter point of view.
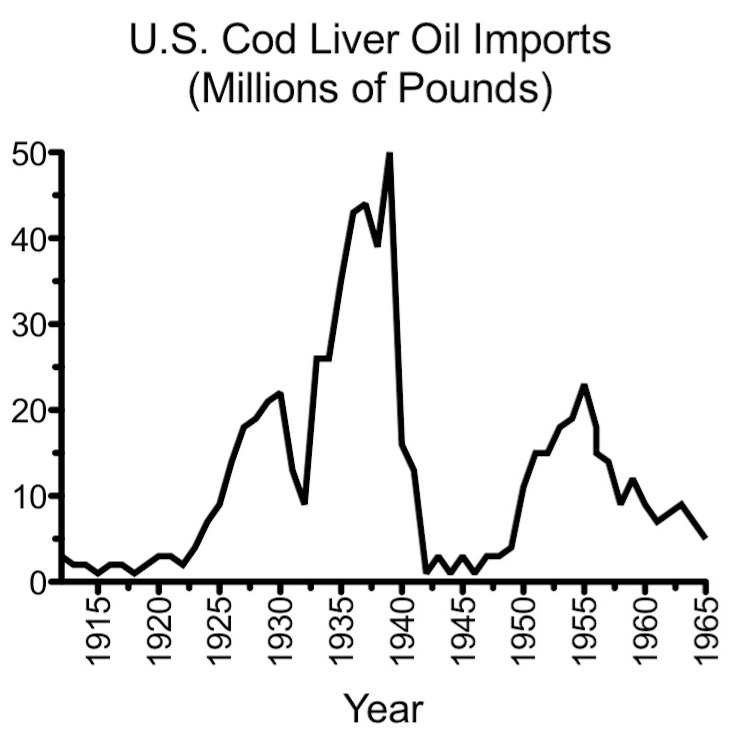
Cod liver oil’s popularity boomed during the “vitamin A as anti-infective” era. To support this, I collected and graphed data for US cod liver oil imports, shown below. Between 1922 and 1939, cod liver oil imports increased 25-fold from two million pounds per year to fifty million pounds per year.
During this boom, manufacturers marketed cod liver oil specifically for its ability to decrease the harmfulness of measles and other infectious diseases. Consider the ad for Squibb cod liver oil below, which focuses on its ability to mitigate the effects of whooping cough, measles, mumps, chicken pox, and scarlet fever.

The text is hard to read because of its size and the resolution of the picture, but here is a quote of some of the text:
Whooping cough, measles, mumps, chicken pox, scarlet fever may do greater harm than most mothers think, but the children have lighter cases, they recover quicker and are less likely to be left with some permanent injury, if they build up good general resistance in advance to fight them. . . . Because cod-liver oil supplies an abundance of vitamin A, doctors recommend it for children daily. It is such a fine resistance builder! In fact, good cod liver oil is one of the richest sources of vitamin A mothers can give. Don’t wait until your child catches one of the “common” diseases. Give him Squibb Cod-Liver Oil now!
This ad focuses on cod liver oil’s ability to reduce the severity of the cases and the likelihood of permanent disabilities resulting from them. It does not address mortality. Conversely, I do not have any data on the severity of cases over time or the rates of infectious disease-related permanent disabilities over time, but I do have data for mortality.
Let us look first at tuberculosis. The graph below is from McKeown’s book and shows tuberculosis mortality for the UK. I have overlaid in red several historical phases related to fat-soluble vitamin nutrition.
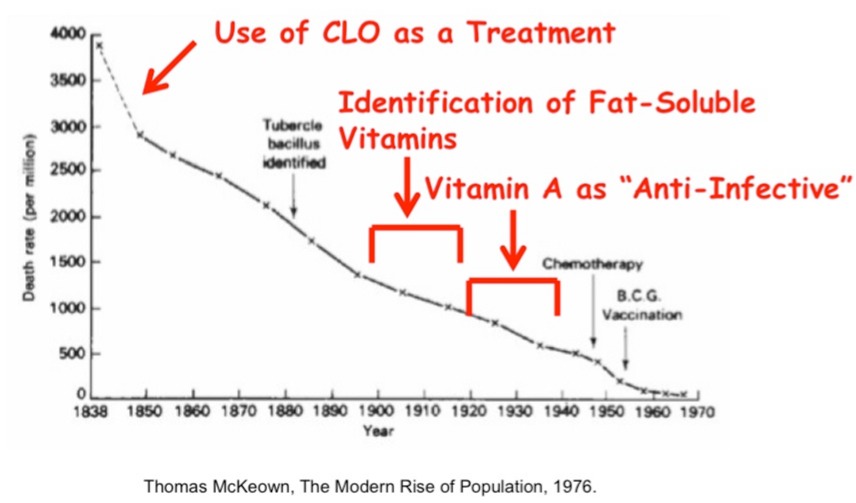
Using McKeown’s data set, we cannot be confident whether the downward trend in tuberculosis began shortly before 1850 or earlier. For all we know, it may have long been in place. Nevertheless, it may also have begun shortly before 1850, which could reflect the initial use of cod liver oil as a treatment for tuberculosis in the early 1840s. I suspect that cod liver oil was used primarily in tuberculosis patients until the turn of the century. As the fat-soluble vitamins were being discovered, I suspect nutritional status improved as the nutritional pioneers began recommending the consumption of nutrient-dense foods. By the time the 25-fold boom in cod liver oil popularity began in the 1920s, tuberculosis mortality was well on its way toward eradication but vitamin A status must certainly have improved throughout that time.
Data for the United States do not go back nearly as far, but they parallel the data for the UK.
It is clear that the downward trend began long before the causal microorganism was discovered and that the trend was almost complete by the time tuberculosis drugs and vaccinations were developed. In the United States, the vaccination never entered the market but mortality was eradicated just the same. Nevertheless, it may be that many of these things made contributions that accumulated over time to ultimately result in eradication. As noted above, Ostry And Frank accepted McKeown’s thesis that improved food ability launched the decline in tuberculosis mortality.
As also noted above, however, Ostry and Frank pointed out that this decline was primarily seen in adolescents and young adults, while the reduction in mortality from other infectious diseases was primarily seen in infants and young children and this latter trend began much later.
Below is shown McKeown’s graph for measles mortality, overlaid with my markings about the historical phases related to fat-soluble vitamin nutrition.

Here the data are striking. Measles mortality suddenly and precipitously declined beginning around 1920 and was essentially eradicated before the vaccine was introduced. Almost the entirety of this decline occurred in the glory days of vitamin A’s anti-infective reputation.
Data for the US are similar. The graph below is noisy because the data are not averaged out over as large intervals so they reflect the episodic nature of measles outbreaks. Nevertheless, if you trace the peaks, the troughs, or an imaginary line through the middle of the data, you can see that eradication occurred along a similar time frame as in the British data.

While it would be overkill to conclude from this that cod liver oil must be the sole explanation for the historical decline in measles mortality, it would be rather foolhardy to ignore its probable contribution. Indeed, clinical trials demonstrated the protective effect of cod liver oil or its fat-soluble vitamins on both measles incidence and mortality; its use increased 25-fold during this time, certainly resulting in widespread increases in vitamin A status; and people used it for the express purpose of rendering infectious diseases, explicitly including measles, less harmful.
It is important to realize that while measles mortality was virtually eradicated prior to the introduction of the vaccine, this is not true of measles incidence. A graph showing that measles incidence was high before the introduction of the vaccine and was virtually eradicated after its introduction can be found here. Unfortunately, these data do not go back earlier than the 1950s, so it is difficult to compare them to the data for measles mortality. To put the incidence data in proper perspective, one must have estimates going back earlier than 1920, and I do not have such data in my possession. Therefore, I do not know if measles incidence declined precipitously beginning around ~1920 like mortality did. If someone has access to data that sheds light on this, please post it in the comments.
It is also important to realize that there is something very important between incidence and mortality: permanent disability. I do not know whether the rates of permanent disability follow the rates of mortality over time, or whether they instead parallel the data on incidence more closely, remaining very high until the vaccine was introduced. This seems critical to put this data in proper perspective: how harmful was measles in the 1950s when the vaccine had not yet been introduced, measles still occurred in relatively large numbers, yet almost no one, compared to the historical norms, died from it? It seems especially unfortunate to not have this data since one of the express purposes for spreading the use of cod liver oil was to reduce the risk of measles-related permanent disability. Again, if you have access to this data, please post it in the comments.
If one peruses pubmed, one will find over a dozen meta-analyses of clinical studies on vitamin A and measles. The data are not consistently supportive. My brief perusal suggests to me modern trials using vitamin A supplements have more consistently shown a benefit for measles incidence than for disability (which is not well investigated) or mortality (which, in the modern era, is presumably better managed than in earlier eras). When interpreting this and other clinical nutrition data we must keep in mind that such investigations almost universally ignore nutrient interactions that should in fact take center stage. I have discussed this at greater length in such articles as “Beyond Good and Evil: Synergy and Context With Dietary Nutrients” and “Nutritional Adjuncts to the Fat-Soluble Vitamins.” I will briefly reiterate a few of the most relevant points here:
- Although Mellanby and Green supported a balanced intake of vitamins A and D, when they dubbed vitamin A the “anti-infective vitamin” this unfortunately led the nutrition science and medical communities to focus exclusively on vitamin A’s role in immunity while ignoring the possibility that vitamin D had a role in immunity that Mellanby and Green failed to uncover. Indeed, I.G. Spiesman later showed in 1941 that vitamins A and D were only capable of reducing the incidence and severity of the common cold when provided in combination with one another.
- Through vitamin A’s regulation of gene expression, it improves the barrier function of epithelial tissues, which is the first line of defense against pathogens. It also increases the production of immune cells, antibodies, and enzymes used by the immune system known as metalloproteinases. All of this depends on zinc: zinc is necessary for the transport of vitamin A in the blood, part of its activation to the metabolite that regulates gene expression, and for the ability of its receptor to bind to DNA and thereby regulate gene expression. Further, some of the vitamin A-regulated metalloproteinases are directly dependent on zinc.
- Vitamin D is also activated to a metabolite that regulates gene expression, and one of that metabolite’s functions is to increase the production of antimicrobial peptides that are toxic to a wide variety of microorganisms. Magnesium is needed for its activation, zinc is needed to allow its receptor to bind to DNA, and, while controversial, vitamin A may be directly involved in allowing vitamin D to regulate gene expression.
- Correcting whatever is the weakest link in an individual will prove most effective. For example, someone who is deficient in zinc but replete in vitamin A will be much more likely to benefit from improving zinc status than improving vitamin A status; if that person could benefit from extra vitamin A, the benefit would probably only occur if the zinc deficiency were also corrected. Such interactions will cause variation within and between clinical studies, and not taking them into account will hamper the interpretation of clinical data.
Thus, the key to improving our understanding beyond the clinical data of the 1920-1940 era is in studying these interactions rather than in reducing the approach to a singular vitamin and generating large amounts of clinical data that can be pooled in meta-analysis. In all likelihood the dietary approach that best promotes robust immunity is one that is diverse, well rounded, and nutrient dense, and one that puts the most emphasis on improving the weakest link in each individual.
I believe these data offer strong support for the hypothesis that cod liver oil played an important role in the eradication of mortality from measles and other infectious diseases. It seems unclear to me how large this contribution is for tuberculosis; it seems likely to be large for measles and perhaps for the other infectious diseases whose mortality declined in parallel with that from measles.
Many discussions focus too narrowly on vaccination. While that topic should not be ignored, I believe that the discussion herein helps broaden the perspective and is a necessary piece of the puzzle.
🖨️ Print post
But vitamin A looks so unscientific and commercial!
But vaccines are scientific and non-commercial. Unlike with cod liver oil, there are no patents involved with vaccines, and they are always safe to everybody. But cod liver oil comes from the liver, which means it will cause gout. And all fish are full of deadly anisakis.
“No patents on vaccines? ”
Of course there are. https://www.commondreams.org/news/2021/04/23/nih-scientist-who-developed-key-vaccine-technology-says-patent-gives-us-leverage
“Vaccines are always safe? ”
You better change your information channels.
https://www.gao.gov/products/gao-15-142
Studies that vitamin d can injures TB also the clo can boost injuring arthritis inflammation
Just out of curiosity, how did acceptance of CLO as a treatment coincide with the discovery of Vitamins A and D? From the graphs it suggested that it they determined it had some positive effect some time earlier than they had a theory as to why. Is that the case?
I just came across your article and thought it was very interesting. You must know by now that Humphries & Bystrianyk plotted US measles incidence from 1913 – 69. Incidence did not drop until the vaccine, although it looks like something was holding it down 1959 – 64: http://www.dissolvingillusions.com/wp-content/uploads/2013/03/G14.8-US-Measles-Incidence-1912-1970-1024×650.png. Incidence and deaths are graphed together here:
https://healthimpactnews.com/wp-content/uploads/sites/2/2013/11/G14.7-US-Measles-RM-1900-1987.png
https://lbrbblog.files.wordpress.com/2014/03/measlesmortalityusa1971-75_1.jpg (from here: https://leftbrainrightbrain.co.uk/2014/03/21/yep-measles-is-still-a-killing-disease/)
https://vaxopedia.files.wordpress.com/2016/10/anti-vax-measles-graph.png (from here but unsourced: https://vaxopedia.org/2016/10/01/graphs-that-show-vaccines-dont-work/)
And here’s a really cool chart that shows measles incidence in every state 1928 – 2003: http://www.linkbanana.com/wp-content/uploads/2014/06/chart-of-measle-vaccine-effectiveness-in-the-us.png (from here: http://www.linkbanana.com/tag/charts/).
The graphs seem to show that mortality was in steep decline many years before the vaccine was introduced but that incidence did not decline as much. If we count a vaccine as an incidence (controlled as opposed to wild) then it probably evens out.
“Incidence did not drop until the vaccine?”
You really need to look at this: https://www.milbank.org/wp-content/uploads/mq/volume-55/issue-03/55-3-The-Questionable-Contribution-of-Medical-Measures-to-the-Decline-of-Mortality-in-the-United-States-in-the-Twentieth-Century.pdf
Vaxopedia is farma sponsord. Lets start with that. So graphs can just be made up.
Secondly how can one know measles incidence did not decline untill vaccin. Their was no rapporting system for measles. So how can one know that the incidence did not decline also?
And how did vaxopedia measure incidence if their is no stats. Explain me that?